

Risk of Human Immunodeficiency Virus Acquisition Among High-Risk Heterosexuals With Nonviral Sexually Transmitted Infections: A Systematic Review and Meta-Analysis
- PMID: 35034049
- PMCID: PMC9133024
- DOI: 10.1097/OLQ.0000000000001601
Risk of Human Immunodeficiency Virus Acquisition Among High-Risk Heterosexuals With Nonviral Sexually Transmitted Infections: A Systematic Review and Meta-Analysis
Abstract
Background: Nonviral sexually transmitted infections (STIs) increase risk of sexually acquired human immunodeficiency virus (HIV) infection. Updated risk estimates carefully scrutinizing temporality bias of studies are needed.
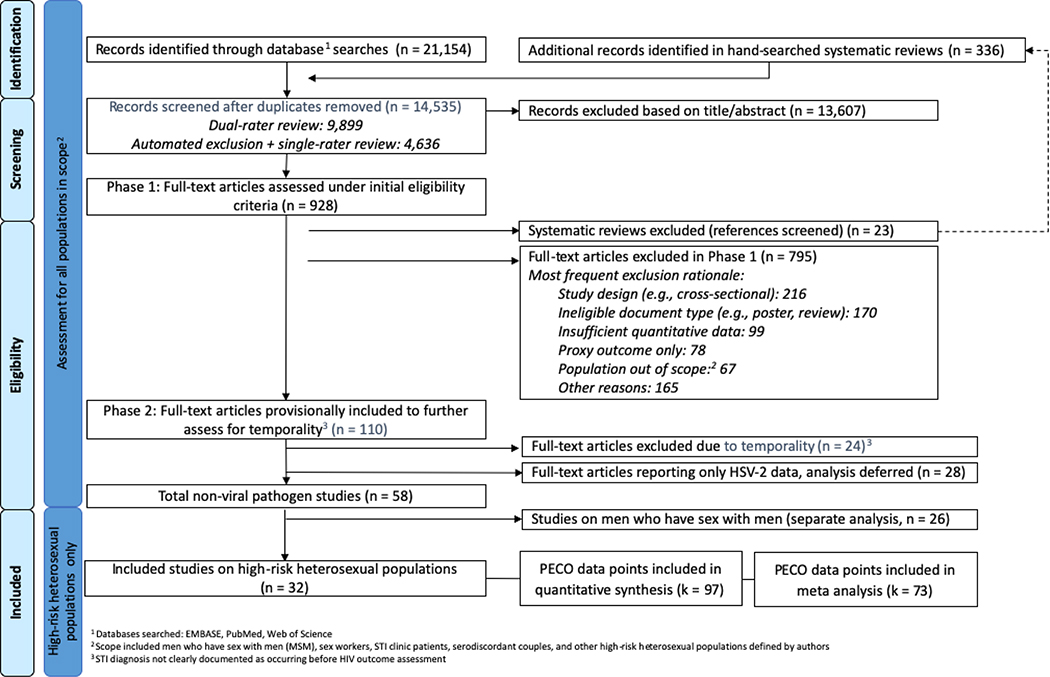
Methods: We conducted a systematic review (PROSPERO CRD42018084299) of peer-reviewed studies evaluating variation in risk of HIV infection among high-risk heterosexuals diagnosed with any of: Chlamydia trachomatis, Mycoplasma genitalium, Neisseria gonorrhoeae, Treponema pallidum, and/or Trichomonas vaginalis. We searched PubMed, Web of Science, and Embase databases through December 2017 and included studies where STIs and HIV were assessed using laboratory tests or medical examinations and where STI was diagnosed before HIV. After dual screening, data extraction, and risk of bias assessment, we meta-analytically pooled risk ratios (RRs).
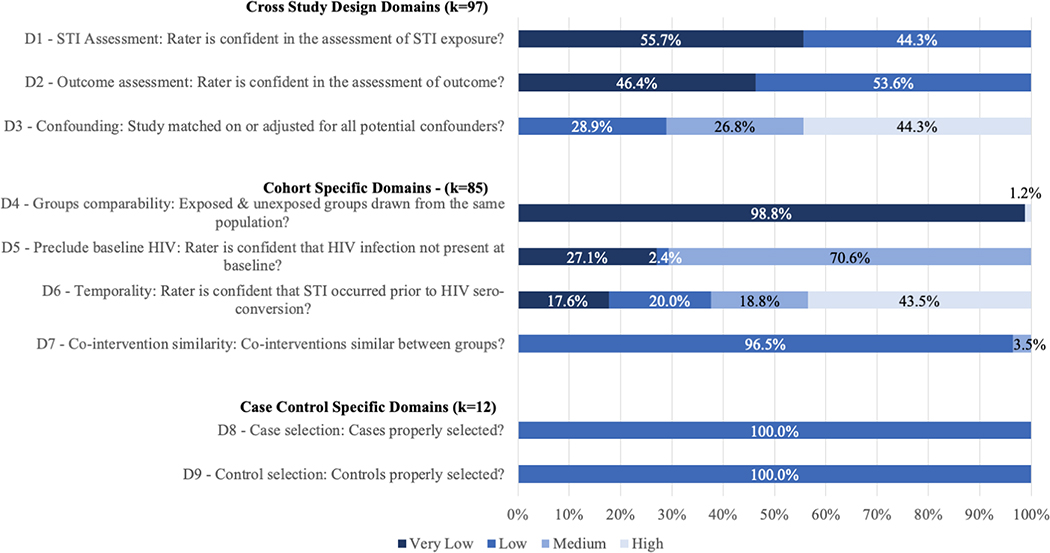
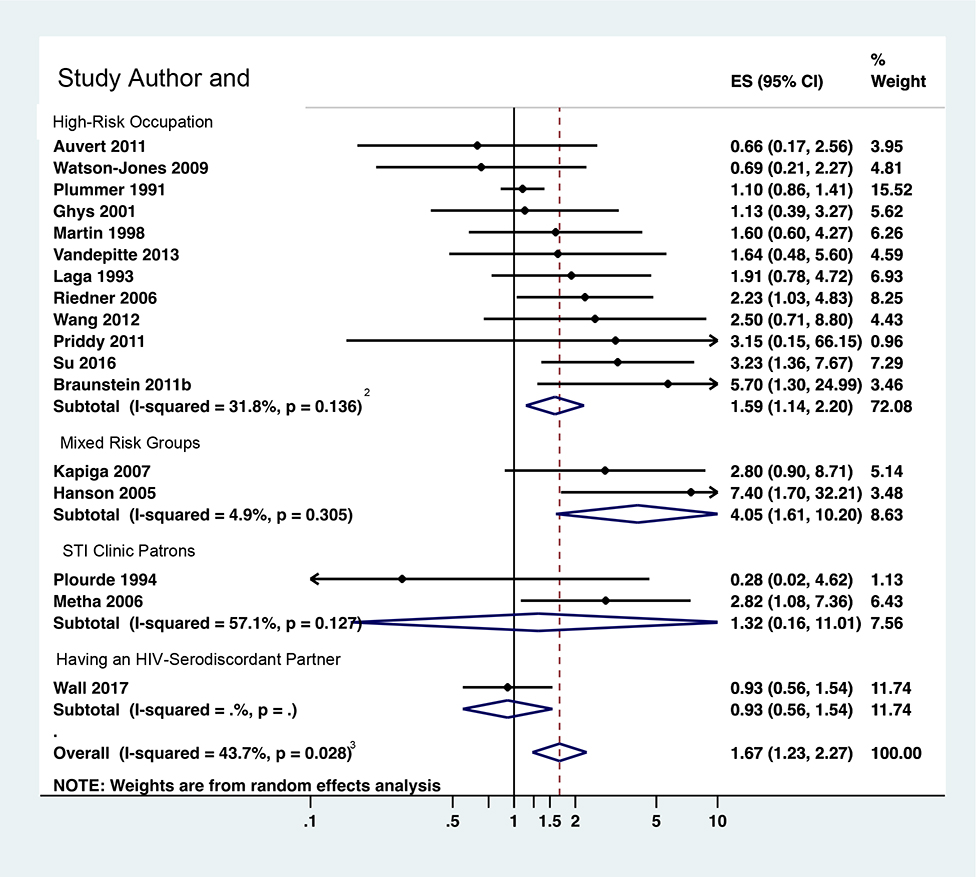
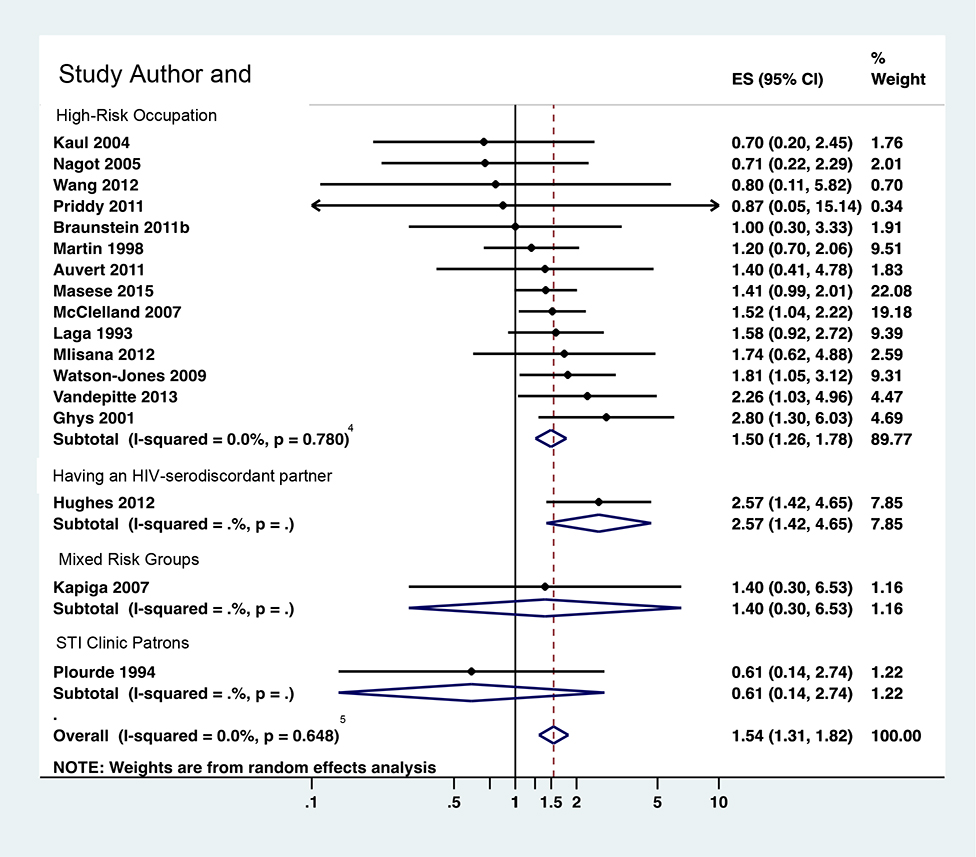
Results: We found 32 eligible studies reporting k = 97 effect size estimates of HIV acquisition risk due to infection with one of the abovementioned STIs. Most data were based on women engaged in sex work or other high-risk occupations in developing countries. Many studies did not measure or adjust for known confounders, including drug injection and condom use, and most were at medium or high risk of bias because of the potential for undetected HIV infection to have occurred before STI infection. Human immunodeficiency virus acquisition risk increased among women infected with any pathogen; the effect was greatest for women infected with Mycoplasma genitalium (RR, 3.10; 95% confidence interval [CI], 1.63-5.92; k = 2) and gonorrhea (RR, 2.81; 95% CI, 2.25-3.50; k = 16) but also statistically significant for women infected with syphilis (RR, 1.67; 95% CI, 1.23-2.27; k = 17), trichomonas (RR, 1.54; 95% CI, 1.31-1.82; k = 17), and chlamydia (RR, 1.49; 95% CI, 1.08-2.04; k = 14). For men, data were space except for syphilis (RR, 1.77; 95% CI, 1.22-2.58; k = 5).
Conclusion: Nonviral STI increases risk of heterosexual HIV acquisition, although uncertainty remains because of risk of bias in primary studies.
Copyright © 2022 American Sexually Transmitted Diseases Association. All rights reserved.
Conflict of interest statement
Conflict of Interest: None declared.
Figures


References
-
- Wasserheit JN. Epidemiological synergy. Interrelationships between human immunodeficiency virus infection and other sexually transmitted diseases. Sexually transmitted diseases 1992; 19(2): 61–77. - PubMed
-
- Rottingen JA, Cameron DW, Garnett GP. A systematic review of the epidemiologic interactions between classic sexually transmitted diseases and HIV: how much really is known? Sexually transmitted diseases 2001; 28(10): 579–97. - PubMed
-
- Sexton J, Garnett G, Rottingen JA. Metaanalysis and metaregression in interpreting study variability in the impact of sexually transmitted diseases on susceptibility to HIV infection. Sexually transmitted diseases 2005; 32(6): 351–7. - PubMed
-
- Freeman EE, Weiss HA, Glynn JR, Cross PL, Whitworth JA, Hayes RJ. Herpes simplex virus 2 infection increases HIV acquisition in men and women: systematic review and meta-analysis of longitudinal studies. AIDS (London, England) 2006; 20(1): 73–83. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
