

Current and future landscape of targeted therapy in HER2-positive advanced breast cancer: redrawing the lines
- PMID: 35035535
- PMCID: PMC8753087
- DOI: 10.1177/17588359211066677
Current and future landscape of targeted therapy in HER2-positive advanced breast cancer: redrawing the lines
Abstract
Background: Evidence to date supports continued human epidermal growth factor receptor 2 (HER2) suppression beyond progression on HER2-directed therapy for advanced HER2-positive breast cancer. Data from several phase II and III trials evaluating HER2-directed therapy following second-line T-DM1 have recently become available.
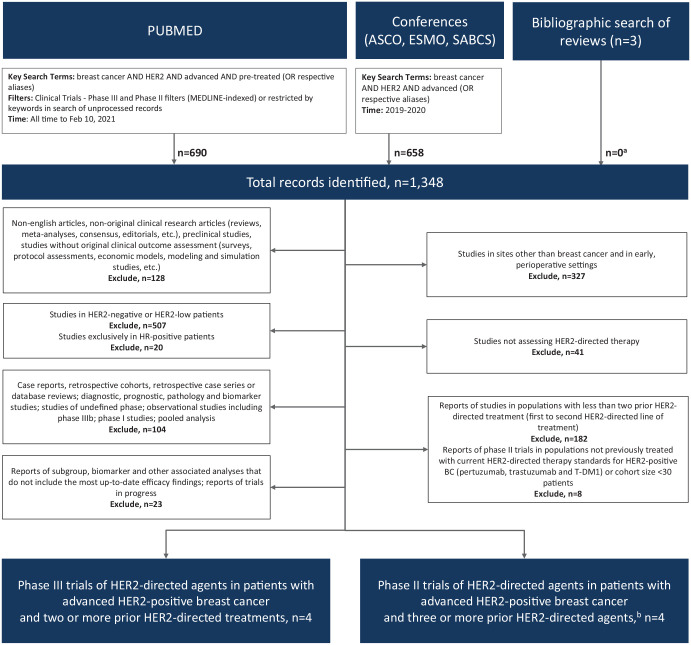
Methods: We performed a systematic search of the published and presented literature to identify phase II and phase III trials assessing novel HER2-targeted agents as third-line therapy or beyond for HER2-positive advanced breast cancer using search terms 'breast cancer' AND 'HER2' AND 'advanced' AND ('phase II' OR 'phase III').
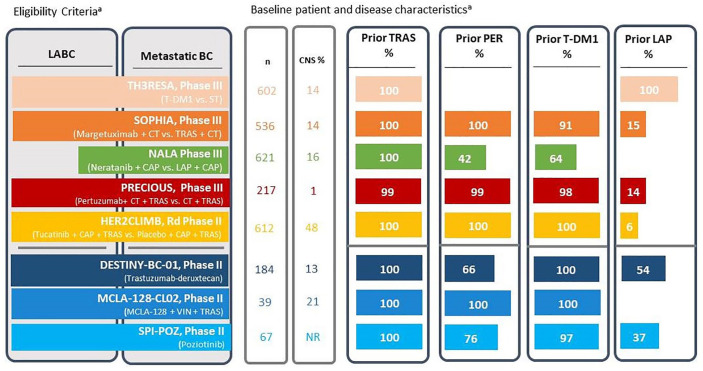
Results: Eight clinical trials reporting efficacy outcomes on third-line or greater HER2-directed therapy for HER2-positive advanced breast cancer were identified. In phase III trials, margetuximab and neratinib combinations demonstrated significant 1.3-month (hazard ratio, HR = 0.71, p < 0.001) and 0.1-month (HR = 0.76, p = 0.006) net improvements in median progression-free survival (PFS), respectively, with no significant improvements in overall survival (OS). Tucatinib added to trastuzumab and capecitabine demonstrated a significant 2.7-month improvement in median PFS (HR = 0.57, p < 0.00001) and a 5.5-month improvement in median OS (HR = 0.73, p = 0.004) in a randomized phase II trial, including significant clinical benefit for patients with brain metastases. Finally, trastuzumab-deruxtecan, zenocutuzumab, and poziotinib demonstrated benefit in phase II trials with the most robust overall response rate (62.0%) and median duration of response (18.2 months) observed for trastuzumab-deruxtecan among heavily pretreated patients.
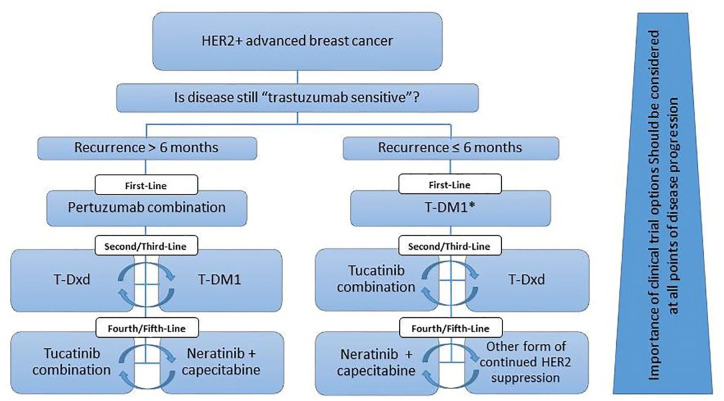
Conclusion: Tucatinib plus trastuzumab and capecitabine significantly prolongs OS, and promising preliminary response outcomes for trastuzumab-deruxtecan suggest that sequencing of these regimens following second-line therapy is reasonable.
Keywords: HER2-positive; T-DM1; T-DXd; advanced disease; breast cancer; neratinib; pertuzumab; trastuzumab; tucatinib.
© The Author(s), 2022.
Conflict of interest statement
Conflict of interest statement: The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Christine Simmons has served in a consultancy or advisory role and received honorarium from Pfizer, Eli Lilly, Roche, and Mylan, and has received research funding from AstraZeneca Global, Roche, Knight Therapeutics, Viatris, and Pfizer. Daniel Rayson has served in a consultancy or advisory role and received honorarium from AstraZeneca, Pfizer, Eli Lilly, Merck, Gilead, Novartis, and Seagen. Anil Abraham Joy has served in a consultancy or advisory role and received honorarium from AstraZeneca, BMS, Eli Lilly, Knight Therapeutics, Gilead, Roche, Novartis, Pfizer, Mylan, and Teva. Jan-Willem Henning has served in a consultancy or advisory role and received honorarium from AstraZeneca, Pfizer, Novartis, Eli Lilly, Roche, Knight Therapeutics, Seagen, and Mylan. Julie Lemieux has served in a consultancy or advisory role and received honorarium from Novartis, Eli Lilly, Gilead, Pfizer, and AstraZeneca, and has received research funding from Celgene, Genentech, GlaxoSmithKline, Roche, Millennium, Novartis, Merck Gilead, Abbvie, Acerta, Bayer, Pfizer, BMS, Esai, Sanofi, Janssen, Ozmosys, Sierra Astrazeneca, and Takeda. Heather McArthur has served in a consultancy or advisory role and received honorarium from Bristol-Myers Squibb, AstraZeneca, Genentech/Roche, Puma Biotechnology, Daiichi-Sankyo, Seattle Genetics, Merck, and Lilly, and has received research funding from Bristol-Myers Squibb, MedImmune, LLC/AstraZenica, BTG, and Merck. Paul B. Card has nothing to declare. Rebecca Dent has served in a consultancy or advisory role and received honorarium from AstraZeneca, Viatris, Pfizer, Eisai, Merck, Eli Lilly, Novartis, and Roche, and has received research funding from AstraZeneca. Christine Brezden-Masley has served in a consultancy or advisory role and received honorarium from AstraZeneca, Eli Lilly, Knight Therapeutics, Mylan, Gilead, Roche, Amgen, Seagen, and Novartis, and has received research funding from Eli Lilly and AstraZeneca.
Figures
References
-
- Sung H, Ferlay J, Siegel RL, et al.. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71: 209–249. - PubMed
-
- Bredin P, Walshe J, Denduluri N. Systemic therapy for metastatic HER2-positive breast cancer. Semin Oncol 2020; 47: 259–269. - PubMed
-
- DeSantis CE, Ma J, Gaudet MM, et al.. Breast cancer statistics, 2019. CA Cancer J Clin 2019; 69: 438–451. - PubMed
-
- Köhler G, Milstein C. Continuous cultures of fused cells secreting antibody of predefined specificity. Nature 1975; 256: 495–497. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
