

Whipple pancreatoduodenectomy: A technical illustration
- PMID: 35036890
- PMCID: PMC8749264
- DOI: 10.1016/j.sopen.2021.11.007
Whipple pancreatoduodenectomy: A technical illustration
Abstract
Background: The Whipple procedure in its current form owes its evolution to the groundbreaking and innovative work of giants in the field of surgery. From being a multistep procedure with high morbidity and mortality, it is now ubiquitously performed in a single setting, often offered via minimally invasive approaches. Training to perform this procedure is an arduous task, and different training paradigms vary significantly.
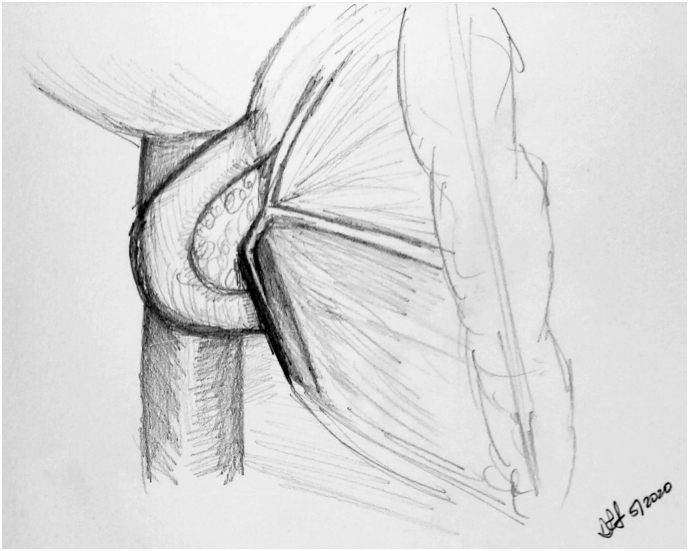
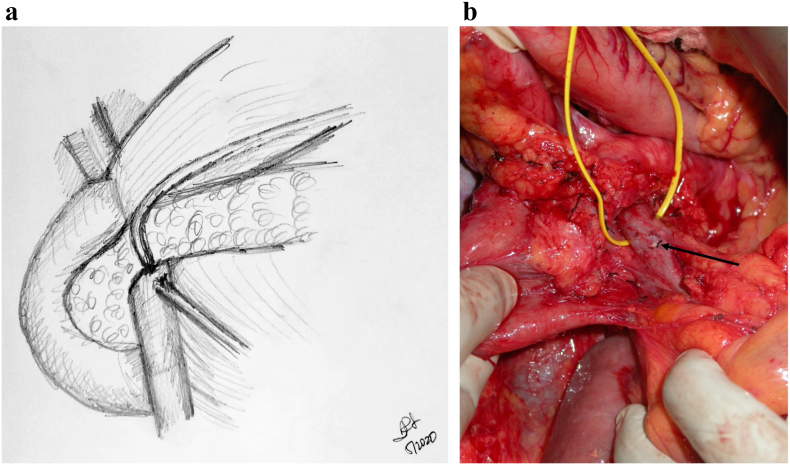
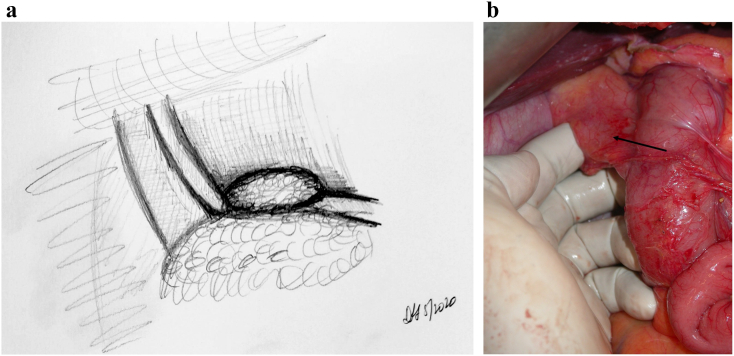
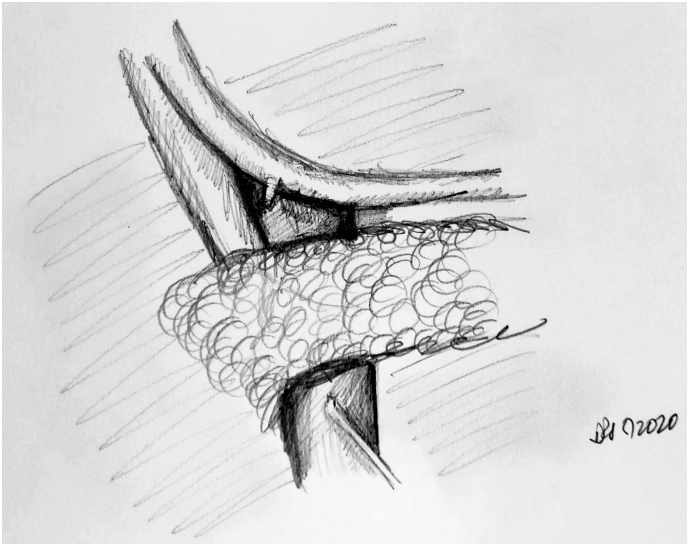
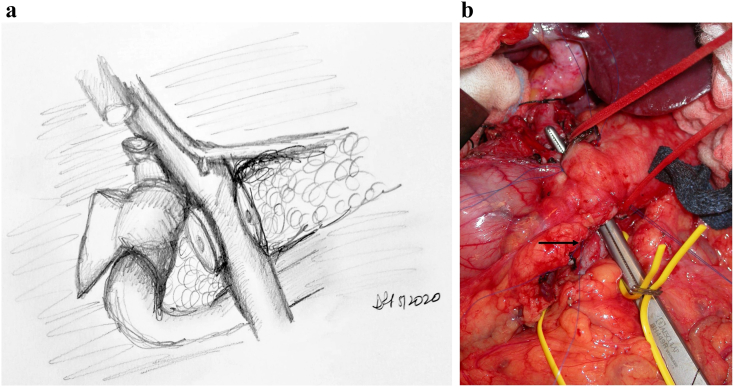
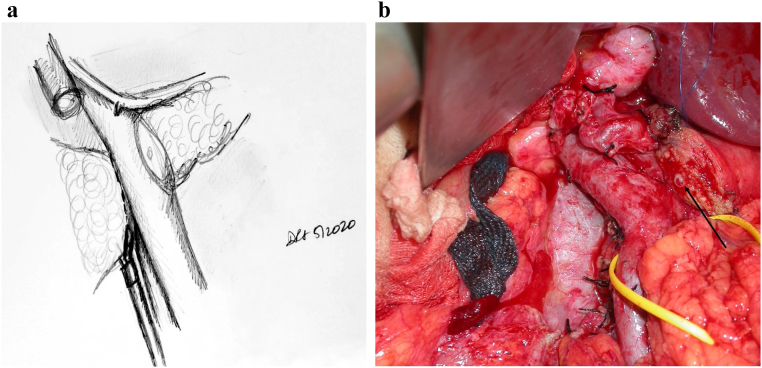
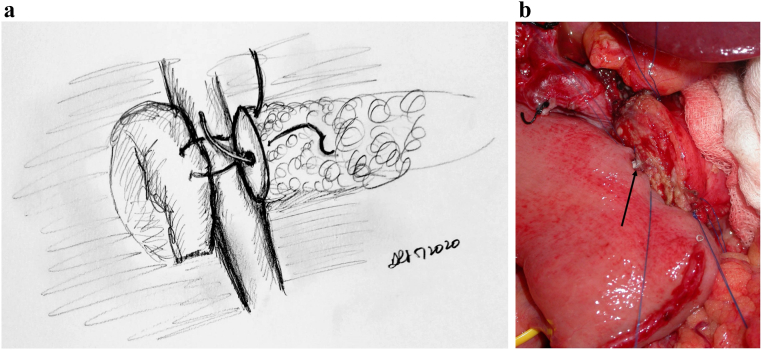
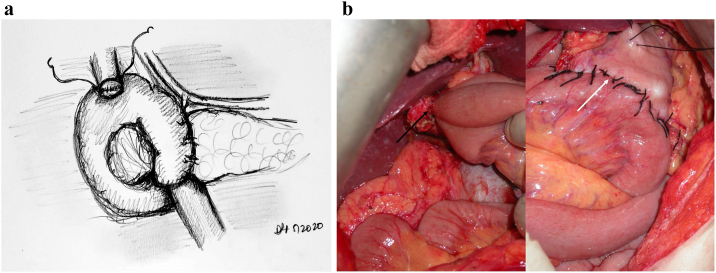
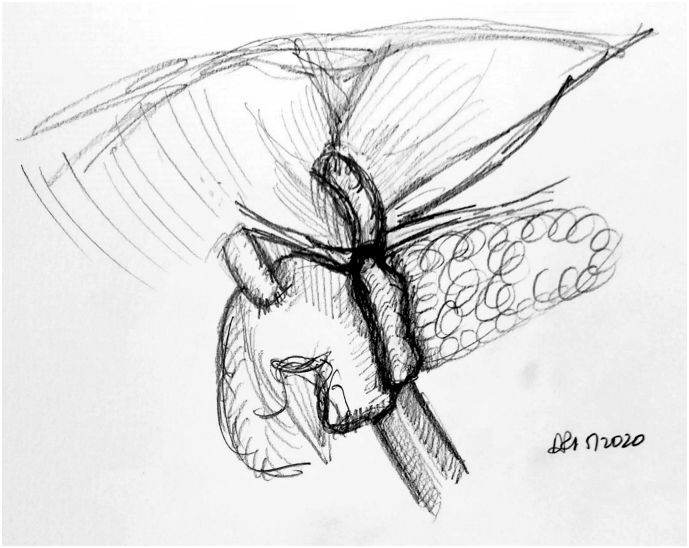
Objectives/methods: The purpose of this paper is to share a standard method by which the surgeon can perform the Whipple procedure in a systematic manner. Using illustrations to make the steps clearer, the authors will postulate that an improvement in mean operative time can be realistically achieved by most pancreatic surgeons. The focus is also on presenting this complex procedure as reproducible and teachable techniques for trainees.
Conclusion: This illustrated review of the Whipple procedure as performed at our institution is intended to help facilitate a streamlined and stepwise progression through what is undoubtedly a challenging surgical procedure. Although the procedure described will not apply to all Whipple operations given the heterogeneity in anatomy and circumstances, our hope is that this will lead to a more efficient procedure and decreased operating room time and costs as well as provide a framework to teach and measure technical progress for surgical trainees.
© 2021 Published by Elsevier Inc.
Figures
References
-
- Howard J.M. History of pancreatic head resection—the evaluation of surgical technique. Am J Surg. 2007;194(4 SUPPL):S6–S10. doi: 10.1016/j.amjsurg.2007.05.029. - DOI
-
- Strasberg S.M., Sanchez L.A., Hawkins W.G., Fields R.C., et al. Resection of tumors of the neck of the pancreas with venous invasion: the “Whipple at the Splenic Artery (WATSA)” procedure. J Gastrintest Surg. 2012;16(5):1048–1054. - PubMed
LinkOut - more resources
Full Text Sources
