

Excessive Blood Pressure Response to Clonidine in Hospitalized Patients With Asymptomatic Severe Hypertension
- PMID: 35038322
- PMCID: PMC9088839
- DOI: 10.1093/ajh/hpac004
Excessive Blood Pressure Response to Clonidine in Hospitalized Patients With Asymptomatic Severe Hypertension
Abstract
Background: There are limited and nonconcordant data on the rapidity and safety of blood pressure response to clonidine in the setting of asymptomatic severe hypertension. We evaluated the blood pressure response to clonidine in hospitalized patients with asymptomatic severe hypertension.
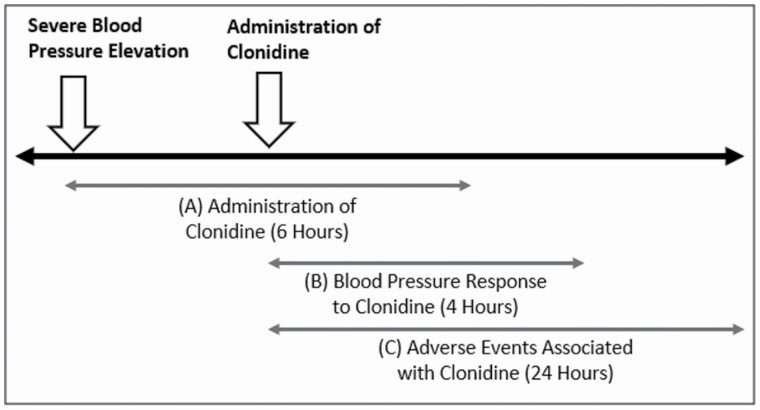
Methods: We performed a review of hospitalized, noncritically ill patients receiving clonidine within 6 hours of developing asymptomatic severe hypertension (systolic blood pressure [SBP] >180 or diastolic blood pressure [DBP] >110 mm Hg in the absence of acute hypertension-mediated target organ damage). The incidence of mean arterial pressure (MAP) reduction by ≥30% at 4 hours after clonidine was the primary endpoint.
Results: We identified 200 relevant patient encounters (median age 63 years, 48.5% women). Median time to clonidine following asymptomatic severe hypertension was 2.8 hours. A total of 20 (10%) patients had ≥30% MAP reduction within 4 hours after clonidine, and 32 (16%) patients had ≥30% reduction in either SBP, DBP, or MAP. Older age, female sex, and preexisting vascular disease were associated with ≥30% MAP reductions (P < 0.05). Only patient sex and clonidine dose of 0.3 mg were significant in multivariable models. There were 14 adverse events observed within 24 hours of administration of clonidine; most (9) were acute kidney injury. There were no ischemic (myocardial, cerebrovascular) events.
Conclusions: A substantial minority of hospitalized patients with asymptomatic severe hypertension experience precipitous blood pressure decline with clonidine, and though blood pressure declines more precipitously in women and those receiving higher doses (0.3 mg specifically), the response to clonidine is generally not predictable on clinical grounds.
Keywords: asymptomatic severe hypertension; blood pressure; clonidine; hypertension; inpatient hypertension.
© The Author(s) 2022. Published by Oxford University Press on behalf of American Journal of Hypertension, Ltd. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures



Comment in
-
Is Clonidine Contraindicated for the Treatment of Hypertensive Urgencies in Hospitalized Patients?Am J Hypertens. 2022 May 10;35(5):391-392. doi: 10.1093/ajh/hpac015. Am J Hypertens. 2022. PMID: 35134819 No abstract available.
References
-
- Lewington S, Clarke R, Qizilbash N, Peto R, Collins R; Prospective Studies Collaboration . Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002; 360:1903–1913. - PubMed
-
- Miura K, Daviglus ML, Dyer AR, Liu K, Garside DB, Stamler J, Greenland P. Relationship of blood pressure to 25-year mortality due to coronary heart disease, cardiovascular diseases, and all causes in young adult men: the Chicago Heart Association Detection Project in Industry. Arch Intern Med 2001; 161:1501–1508. - PubMed
-
- Astarita A, Covella M, Vallelonga F, Cesareo M, Totaro S, Ventre L, Aprà F, Veglio F, Milan A. Hypertensive emergencies and urgencies in emergency departments: a systematic review and meta-analysis. J Hypertens 2020; 38:1203–1210. - PubMed
-
- Peixoto AJ. Acute severe hypertension. N Engl J Med 2019; 381:1843–1852. - PubMed
-
- Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, DePalma SM, Gidding S, Jamerson KA, Jones DW, MacLaughlin EJ, Muntner P, Ovbiagele B, Smith SC Jr, Spencer CC, Stafford RS, Taler SJ, Thomas RJ, Williams KA Sr, Williamson JD, Wright JT Jr. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018; 71:1269–1324. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
