

Injection Guidelines for Treating Midface Volume Deficiency With Hyaluronic Acid Fillers: The ATP Approach (Anatomy, Techniques, Products)
- PMID: 35039828
- PMCID: PMC9373948
- DOI: 10.1093/asj/sjac007
Injection Guidelines for Treating Midface Volume Deficiency With Hyaluronic Acid Fillers: The ATP Approach (Anatomy, Techniques, Products)
Abstract
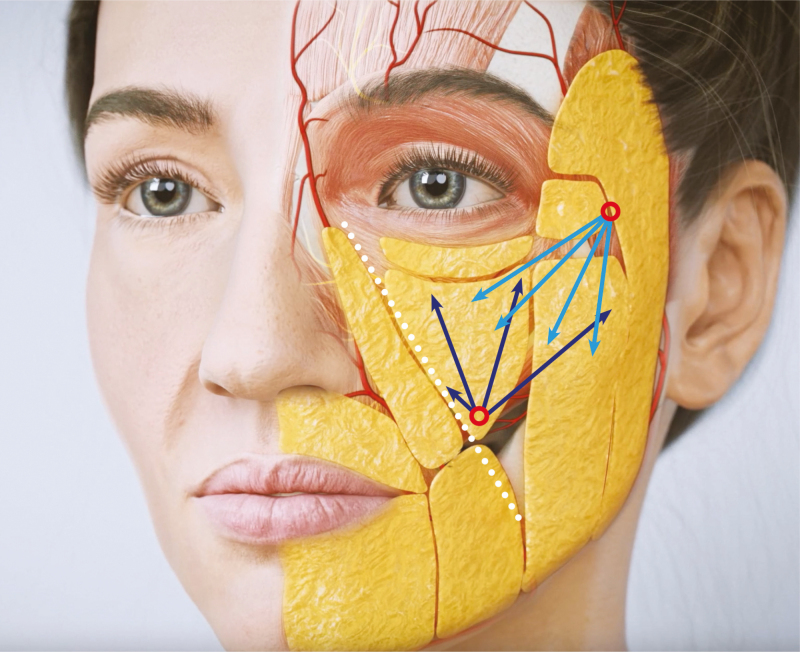
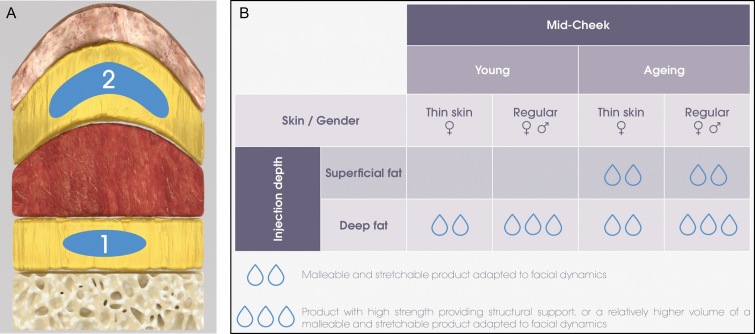
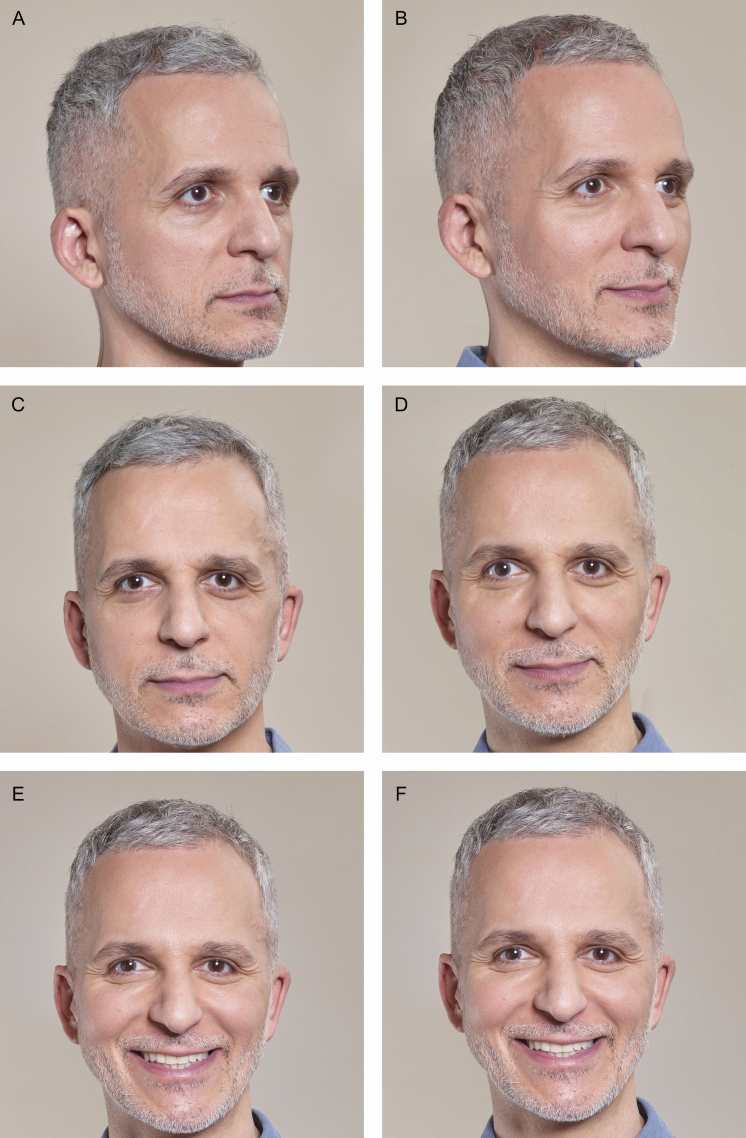
Midface rejuvenation is among the most valuable indications of hyaluronic acid dermal fillers, because malar projection and full upper cheeks significantly contribute to a youthful appearance. Hyaluronic acid fillers have evolved over the past 2 decades to meet specific clinical needs such as strong projection capacity and adaptability to facial dynamism. As a result, they now represent the treatment of choice for midface rejuvenation throughout age ranges by offering the potential for noninvasive treatment, immediate results, and minimal downtime. Because the 5-layered structure of the midface plays a central role in the human face, injecting the midface area may also indirectly improve other aesthetic concerns such as infraorbital hollowing and nasolabial folds. Nonetheless, midface rejuvenation requires a tailored treatment approach and a thorough knowledge of anatomy to minimize procedural risks and achieve natural-looking results. This article provides an extensive anatomical description of the midface and of the usual course and depth of vascular structures circulating nearby to delineate a treatment area and minimize procedural risks. Furthermore, considering the differential mobility and mechanical constraints of each layer of the midface, a multilayer treatment algorithm is proposed for adapting the treatment strategy to patient specificities (including age, gender, skin type, and morphology). Emphasis is also placed on desirable filler properties to create deep structural support on the one hand and accompany facial movement on the other hand.
© 2022 The Aesthetic Society.
Figures






Comment in
-
Commentary on: Injection Guidelines for Treating Midface Volume Deficiency With Hyaluronic Acid Fillers: The ATP Approach (Anatomy, Techniques, Products).Aesthet Surg J. 2022 Aug 1;42(8):935-936. doi: 10.1093/asj/sjac041. Aesthet Surg J. 2022. PMID: 35511146 No abstract available.
References
-
- de Maio M, DeBoulle K, Braz A, Rohrich RJ. Facial assessment and injection guide for botulinum toxin and injectable hyaluronic acid fillers: focus on the midface. Plast Reconstr Surg. 2017;140(4):540e-550e. - PubMed
-
- Monheit GD. Nonsurgical facial rejuvenation. Facial Plast Surg. 2014;30(4):462-467. - PubMed
-
- Pontius AT, Chaiet SR, Williams EF 3rd. Midface injectable fillers: have they replaced midface surgery? Facial Plast Surg Clin North Am. 2013;21(2):229-239. - PubMed
-
- National Plastic Surgery Statistics 2020. American Society of Plastic Surgeons. Accessed September 3, 2021. https://www.plasticsurgery.org/documents/News/Statistics/2020/plastic-su...
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
