

Endoscopic vacuum therapy in the upper gastrointestinal tract: when and how to use it
- PMID: 35041047
- PMCID: PMC9151563
- DOI: 10.1007/s00423-022-02436-5
Endoscopic vacuum therapy in the upper gastrointestinal tract: when and how to use it
Abstract
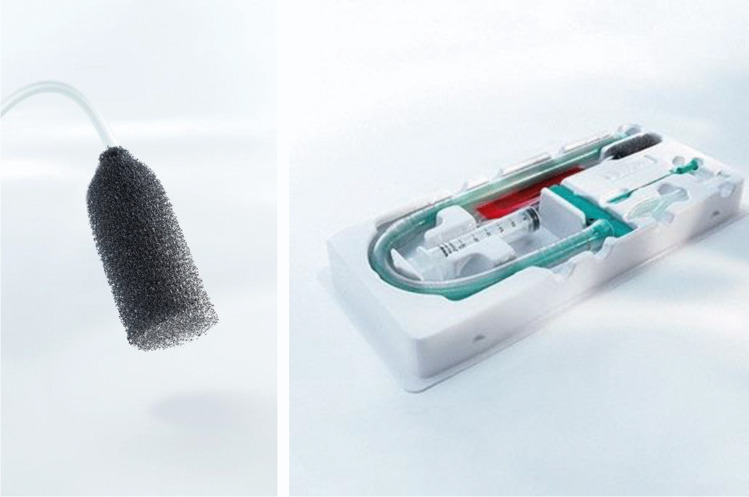
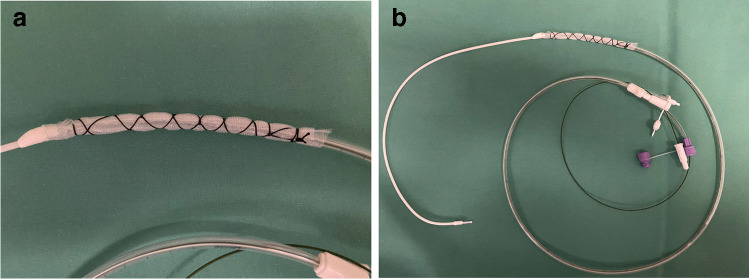
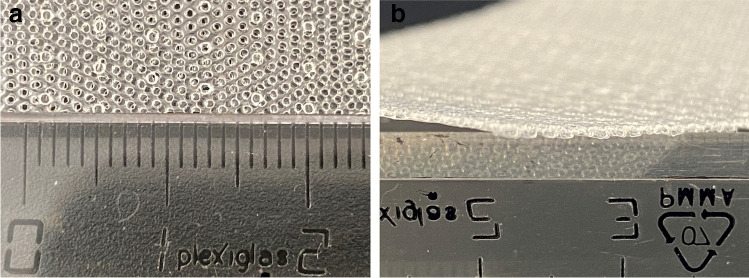
Background: Endoscopic vacuum therapy (EVT) has emerged as a novel treatment option for upper gastrointestinal wall defects. The basic principle of action of EVT entails evacuation of secretions, removal of wound debris, and containment of the defect. Furthermore, there is increasing evidence that EVT reduces interstitial edema, increases oxygen saturation, and promotes tissue granulation and microcirculation. Various devices, such as macroporous polyurethane sponge systems or open-pore film drains, have been developed for specific indications. Depending on the individual situation, EVT devices can be placed in- or outside the intestinal lumen, as a stand-alone procedure, or in combination with surgical, radiological, and other endoscopic interventions.
Purpose: The aim of this narrative review is to describe the current spectrum of EVT in the upper gastrointestinal tract and to assess and summarize the related scientific literature.
Conclusions: There is growing evidence that the efficacy of EVT for upper GI leakages exceeds that of other interventional treatment modalities such as self-expanding metal stents, clips, or simple drainages. Owing to the promising results and the excellent risk profile, EVT has become the therapy of choice for perforations and anastomotic leakages of the upper gastrointestinal tract in many centers of expertise. In addition, recent clinical research suggests that preemptive use of EVT after high-risk upper gastrointestinal resections may play an important role in reducing postoperative morbidity.
Keywords: Anastomotic leakage; Endoscopic vacuum therapy; Esophageal perforation; Esophagectomy; Gastrectomy; Negative pressure therapy.
© 2022. The Author(s).
Conflict of interest statement
CAG received a research grant from B. Braun Melsungen AG, Melsungen, Germany. The other authors declare that they have no conflict of interest.
Figures




References
-
- Sartre J-P (1943) L’Etreet le Néant; Essai D’Ontologie Phenomenologique. Gallimard Paris
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
