

Effects of preconception lifestyle intervention in infertile women with obesity: The FIT-PLESE randomized controlled trial
- PMID: 35041662
- PMCID: PMC8765626
- DOI: 10.1371/journal.pmed.1003883
Effects of preconception lifestyle intervention in infertile women with obesity: The FIT-PLESE randomized controlled trial
Abstract
Background: Women with obesity and infertility are counseled to lose weight prior to conception and infertility treatment to improve pregnancy rates and birth outcomes, although confirmatory evidence from randomized trials is lacking. We assessed whether a preconception intensive lifestyle intervention with acute weight loss is superior to a weight neutral intervention at achieving a healthy live birth.
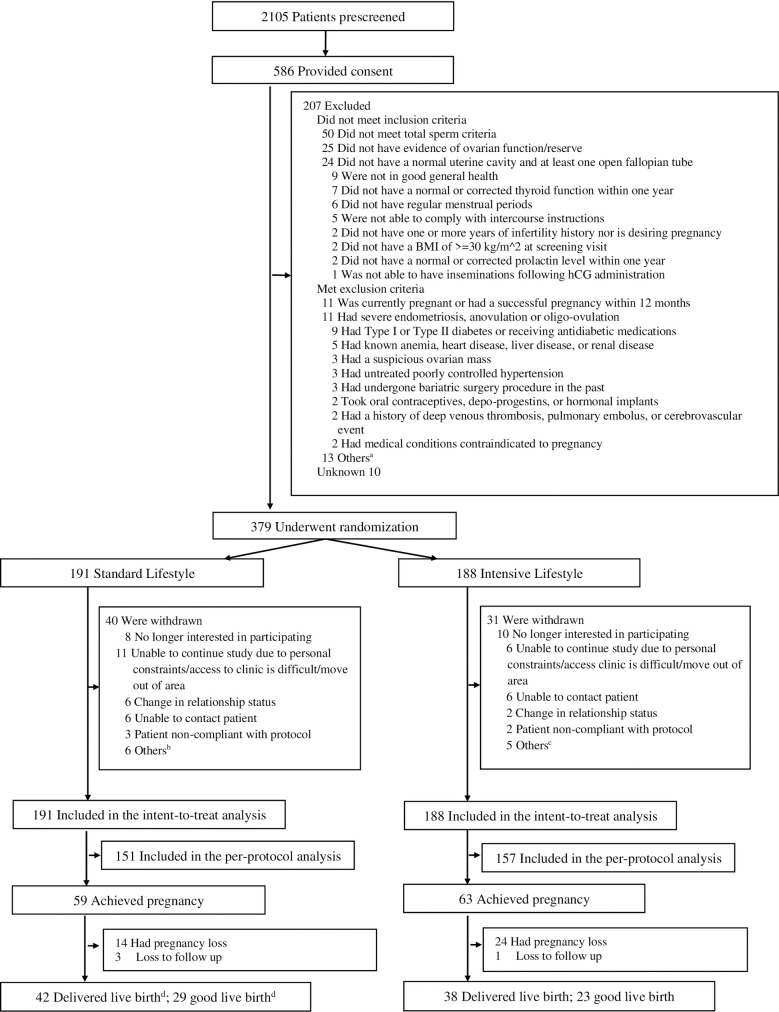
Methods and findings: In this open-label, randomized controlled study (FIT-PLESE), 379 women with obesity (BMI ≥ 30 kg/m2) and unexplained infertility were randomly assigned in a 1:1 ratio to 2 preconception lifestyle modification groups lasting 16 weeks, between July 2015 and July 2018 (final follow-up September 2019) followed by infertility therapy. The primary outcome was the healthy live birth (term infant of normal weight without major anomalies) incidence. This was conducted at 9 academic health centers across the United States. The intensive group underwent increased physical activity and weight loss (target 7%) through meal replacements and medication (Orlistat) compared to a standard group with increased physical activity alone without weight loss. This was followed by standardized empiric infertility treatment consisting of 3 cycles of ovarian stimulation/intrauterine insemination. Outcomes of any resulting pregnancy were tracked. Among 191 women randomized to standard lifestyle group, 40 dropped out of the study before conception; among 188 women randomized to intensive lifestyle group, 31 dropped out of the study before conception. All the randomized women were included in the intent-to-treat analysis for primary outcome of a healthy live birth. There were no significant differences in the incidence of healthy live births [standard 29/191(15.2%), intensive 23/188(12.2%), rate ratio 0.81 (0.48 to 1.34), P = 0.40]. Intensive had significant weight loss compared to standard (-6.6 ± 5.4% versus -0.3 ± 3.2%, P < 0.001). There were improvements in metabolic health, including a marked decrease in incidence of the metabolic syndrome (baseline to 16 weeks: standard: 53.6% to 49.4%, intensive 52.8% to 32.2%, P = 0.003). Gastrointestinal side effects were significantly more common in intensive. There was a higher, but nonsignificant, first trimester pregnancy loss in the intensive group (33.3% versus 23.7% in standard, 95% rate ratio 1.40, 95% confidence interval [CI]: 0.79 to 2.50). The main limitations of the study are the limited power of the study to detect rare complications and the design difficulty in finding an adequate time matched control intervention, as the standard exercise intervention may have potentially been helpful or harmful.
Conclusions: A preconception intensive lifestyle intervention for weight loss did not improve fertility or birth outcomes compared to an exercise intervention without targeted weight loss. Improvement in metabolic health may not translate into improved female fecundity.
Trial registration: ClinicalTrials.gov NCT02432209.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: R.S.L reports consulting fees from InSupp, Ferring, Bayer, Abbvie and Fractyl and research sponsorship from Guerbet and the NIH (U10 HD38992). K.R.H. reports research support from Roche Diagnostics, Ferring and Ablacare and the NIH (U10HD077680). M.P.D reports institutional grants/contracts from Bayer, ObsEva, and AbbVie; serving as a member of the Board of Directors and a stockholder of Advanced Reproductive Care; and serving as a Consultant for Seikagaku, Actamax, AEGEA, Temple Therapeutics, and ARC Medical Devices as well as receiving funding from the NIH(U10 HD39005). A.Z.S. reports consulting fees from Seikagaku and Prima-Temp and research funding from the NIH. M.I.C. reports research funding from Ferring Pharmaceuticals and the NIH (U10HD077844). C.C. reports research funding from the NIH (U10 HD27049). R.A.W. reports Ablacare PCOS, Amgen Repatha in Pg and Partners Mass General Menopause Reviews, grants from NICHD. S.A.K. reports research grant from Merck. D.B.S. reports grants from National Institute of Diabetes, Digestive and Kidney Disease, National Institute of Dental and Craniofacial Research, Department of Defense and Commonwealth of Pennsylvania (PA CURE), consulting fees from Ethicon and NovoNordisk. N.S. reports consulting for Ansh Labs, and is a Scientific Advisor to Astellas and Menogenix, Inc. H.Z. reports research funding from the NIH (U10HD055925).
Figures
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
