

Telehealth Management and Risk Stratification of Older Patients With Chronic Heart Failure During COVID-19 Pandemic: Prognostic Evaluation of the TeleHFCovid19-Score
- PMID: 35041828
- PMCID: PMC8702408
- DOI: 10.1016/j.jamda.2021.12.024
Telehealth Management and Risk Stratification of Older Patients With Chronic Heart Failure During COVID-19 Pandemic: Prognostic Evaluation of the TeleHFCovid19-Score
Abstract
Objectives: To evaluate 6-month risk stratification capacity of the newly developed TeleHFCovid19-Score for remote management of older patients with heart failure (HF) during the coronavirus disease 2019 pandemic.
Design: Monocentric observational prospective study.
Setting and participants: Older HF outpatients remotely managed during the first pandemic wave.
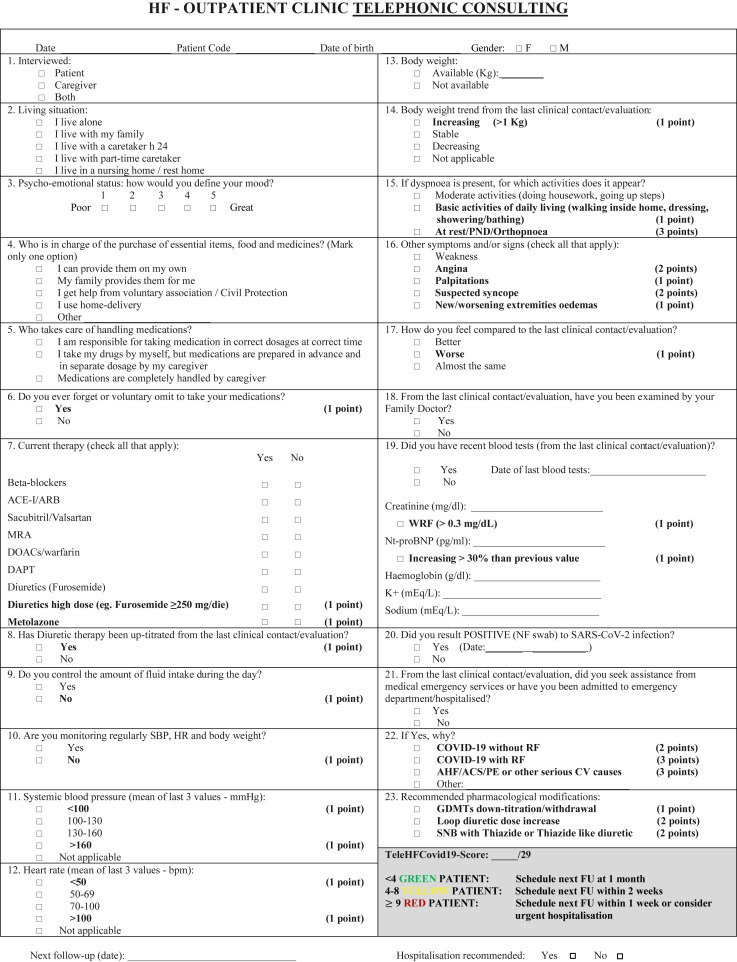
Methods: The TeleHFCovid19-Score (0-29) was obtained by an ad hoc developed multiparametric standardized questionnaire administered during telephone visits to older HF patients (and/or caregivers) followed at our HF clinic. Questions were weighed on the basis of clinical judgment and review of current HF literature. According to the score, patients were divided in progressively increasing risk groups: green (0-3), yellow (4-8), and red (≥9).
Results: A total of 146 patients composed our study population: at baseline, 112, 21, and 13 were classified as green, yellow, and red, respectively. Mean age was 81±9 years, and women were 40%. Compared to patients of red and yellow groups, those in the green group had a lower use of high-dose loop diuretics (P < .001) or thiazide-like diuretics (P = .027) and had reported less frequently dyspnea at rest or for basic activities, new or worsening extremity edema, or weight increase (all P < .001). At 6 months, compared with red (62.2%) and yellow patients (33.3%), green patients (8.9%) presented a significantly lower rate of the composite outcome of cardiovascular death and/or HF hospitalization (P < .001). Moreover, receiver operating characteristic curve analysis showed a high sensibility and specificity of our score at 6 months (area under the curve = 0.789, 95% CI 0.682-0.896, P < .001) with a score <4.5 (very close to green group cutoff) that identified lower-risk subjects.
Conclusions and implications: The TeleHFCovid19-Score was able to correctly identify patients with midterm favorable outcome. Therefore, our questionnaire might be used to identify low-risk chronic HF patients who could be temporarily managed remotely, allowing to devote more efforts to the care of higher-risk patients who need closer and on-site clinical evaluations.
Keywords: COVID-19; Heart failure; SARS-CoV-2; pandemic; telehealth; telemedicine.
Copyright © 2021 AMDA – The Society for Post-Acute and Long-Term Care Medicine. Published by Elsevier Inc. All rights reserved.
Figures


References
-
- Feltner C., Jones C.D., Cené C.W., et al. Transitional care interventions to prevent readmissions for persons with heart failure. Ann Intern Med. 2014;160:774–784. - PubMed
-
- Koehler F., Winkler S., Schieber M., et al. Telemedical interventional monitoring in heart failure investigators. Impact of remote telemedical management on mortality and hospitalizations in ambulatory patients with chronic heart failure: the Telemedical Interventional Monitoring in Heart Failure Study. Circulation. 2011;123:1873–1880. - PubMed
-
- Jerant A.F., Azari R., Martinez C., et al. A randomized trial of telenursing to reduce hospitalization for heart failure: patient-centered outcomes and nursing indicators. Home Health Care Serv Q. 2003;22:1–20. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
