

Clinical outcomes in individuals at clinical high risk of psychosis who do not transition to psychosis: a meta-analysis
- PMID: 35042573
- PMCID: PMC8786617
- DOI: 10.1017/S2045796021000639
Clinical outcomes in individuals at clinical high risk of psychosis who do not transition to psychosis: a meta-analysis
Abstract
Aims: The clinical outcomes of individuals at clinical high risk of psychosis (CHR-P) who do not transition to psychosis are heterogeneous and inconsistently reported. We aimed to comprehensively evaluate longitudinally a wide range of outcomes in CHR-P individuals not developing psychosis.
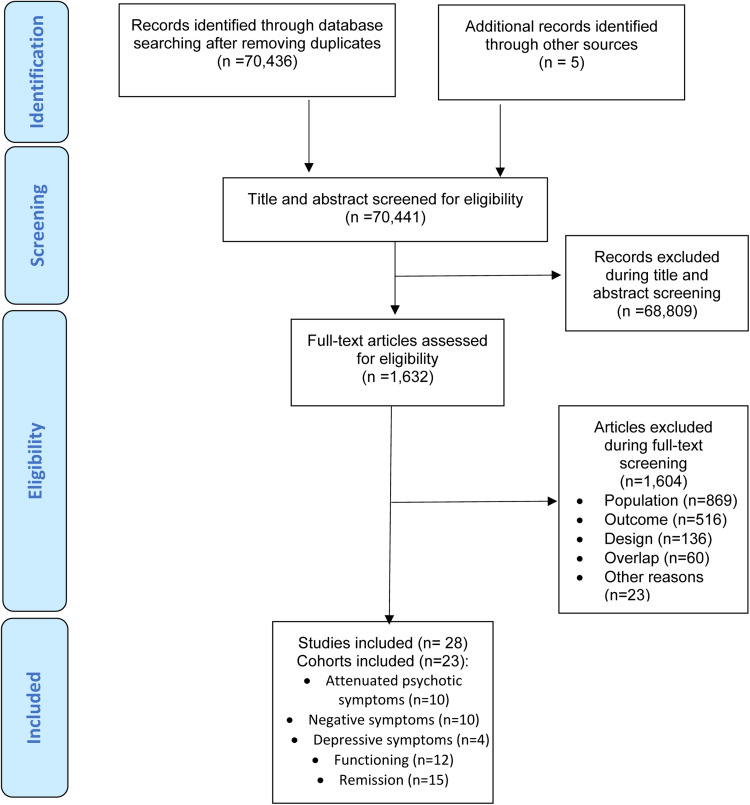
Methods: "Preferred Reporting Items for Systematic reviews and Meta-Analyses" and "Meta-analysis Of Observational Studies in Epidemiology"-compliant meta-analysis (PROSPERO: CRD42021229212) searching original CHR-P longitudinal studies in PubMed and Web of Science databases up to 01/11/2021. As primary analysis, we evaluated the following outcomes within CHR-P non-transitioning individuals: (a) change in the severity of attenuated psychotic symptoms (Hedge's g); (b) change in the severity of negative psychotic symptoms (Hedge's g); (c) change in the severity of depressive symptoms (Hedge's g); (d) change in the level of functioning (Hedge's g); (e) frequency of remission (at follow-up). As a secondary analysis, we compared these outcomes in those CHR-P individuals who did not transition vs. those who did transition to psychosis at follow-up. We conducted random-effects model meta-analyses, sensitivity analyses, heterogeneity analyses, meta-regressions and publication bias assessment. The risk of bias was assessed using a modified version of the Newcastle-Ottawa Scale (NOS).
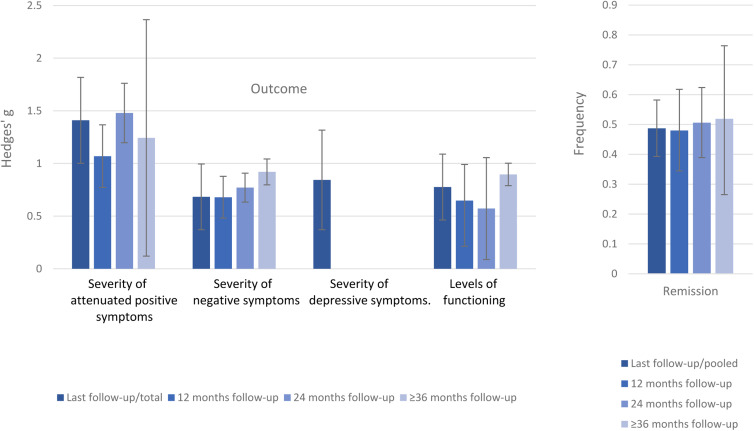
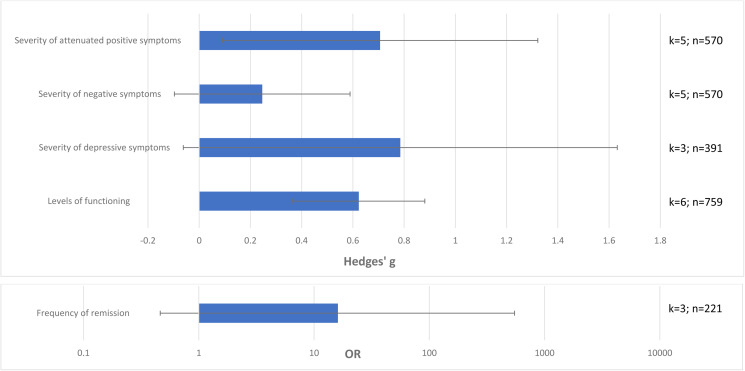
Results: Twenty-eight studies were included (2756 CHR-P individuals, mean age = 20.4, 45.5% females). The mean duration of follow-up of the included studies was of 30.7 months. Primary analysis: attenuated psychotic symptoms [Hedges' g = 1.410, 95% confidence interval (CI) 1.002-1.818]; negative psychotic symptoms (Hedges' g = 0.683, 95% CI 0.371-0.995); depressive symptoms (Hedges' g = 0.844, 95% CI 0.371-1.317); and functioning (Hedges' g = 0.776, 95% CI 0.463-1.089) improved in CHR-P non-transitioning individuals; 48.7% remitted at follow-up (95% CI 39.3-58.2%). Secondary analysis: attenuated psychotic symptoms (Hedges' g = 0.706, 95% CI 0.091-1.322) and functioning (Hedges' g = 0.623, 95% CI 0.375-0.871) improved in CHR-P individuals not-transitioning compared to those transitioning to psychosis, but there were no differences in negative or depressive symptoms or frequency of remission (p > 0.05). Older age was associated with higher improvements of attenuated psychotic symptoms (β = 0.225, p = 0.012); publication years were associated with a higher improvement of functioning (β = -0.124, p = 0.0026); a lower proportion of Brief Limited Intermittent Psychotic Symptoms was associated with higher frequencies of remission (β = -0.054, p = 0.0085). There was no metaregression impact for study continent, the psychometric instrument used, the quality of the study or proportion of females. The NOS scores were 4.4 ± 0.9, ranging from 3 to 6, revealing the moderate quality of the included studies.
Conclusions: Clinical outcomes improve in CHR-P individuals not transitioning to psychosis but only less than half remit over time. Sustained clinical attention should be provided in the longer term to monitor these outcomes.
Keywords: Psychosis; clinical high risk; clinical outcomes; meta-analysis; progression; transition.
Conflict of interest statement
Dr Salazar de Pablo has received honoraria from Janssen Cilag. Professor Fusar-Poli has received research fees from Lundbeck and honoraria from Lundbeck, Angelini, Menarini and Boehringer Ingelheim outside the current study.
Figures
References
-
- Addington J, Stowkowy J, Liu L, Cadenhead KS, Cannon TD, Cornblatt BA, McGlashan TH, Perkins DO, Seidman LJ, Tsuang MT, Walker EF, Bearden CE, Mathalon DH, Santesteban-Echarri O and Woods SW (2019) Clinical and functional characteristics of youth at clinical high-risk for psychosis who do not transition to psychosis. Psychological Medicine 49, 1670–1677. - PubMed
-
- Albert U, Tomassi S, Maina G and Tosato S (2018) Prevalence of non-psychotic disorders in ultra-high risk individuals and transition to psychosis: a systematic review. Psychiatry Research 270, 1–12. - PubMed
-
- American Psychiatric Association (2013) Diagnostic and Statistical Manual of Mental Disorders. Washington, DC: American Psychiatric Association.
-
- Armando M, Pontillo M, De Crescenzo F, Mazzone L, Monducci E, Lo Cascio N, Santonastaso O, Pucciarini ML, Vicari S, Schimmelmann BG and Schultze-Lutter F (2015) Twelve-month psychosis-predictive value of the ultra-high risk criteria in children and adolescents. Schizophrenia Research 169, 186–192. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
