

Primary hypothyroidism and quality of life
- PMID: 35042968
- PMCID: PMC8930682
- DOI: 10.1038/s41574-021-00625-8
Primary hypothyroidism and quality of life
Abstract
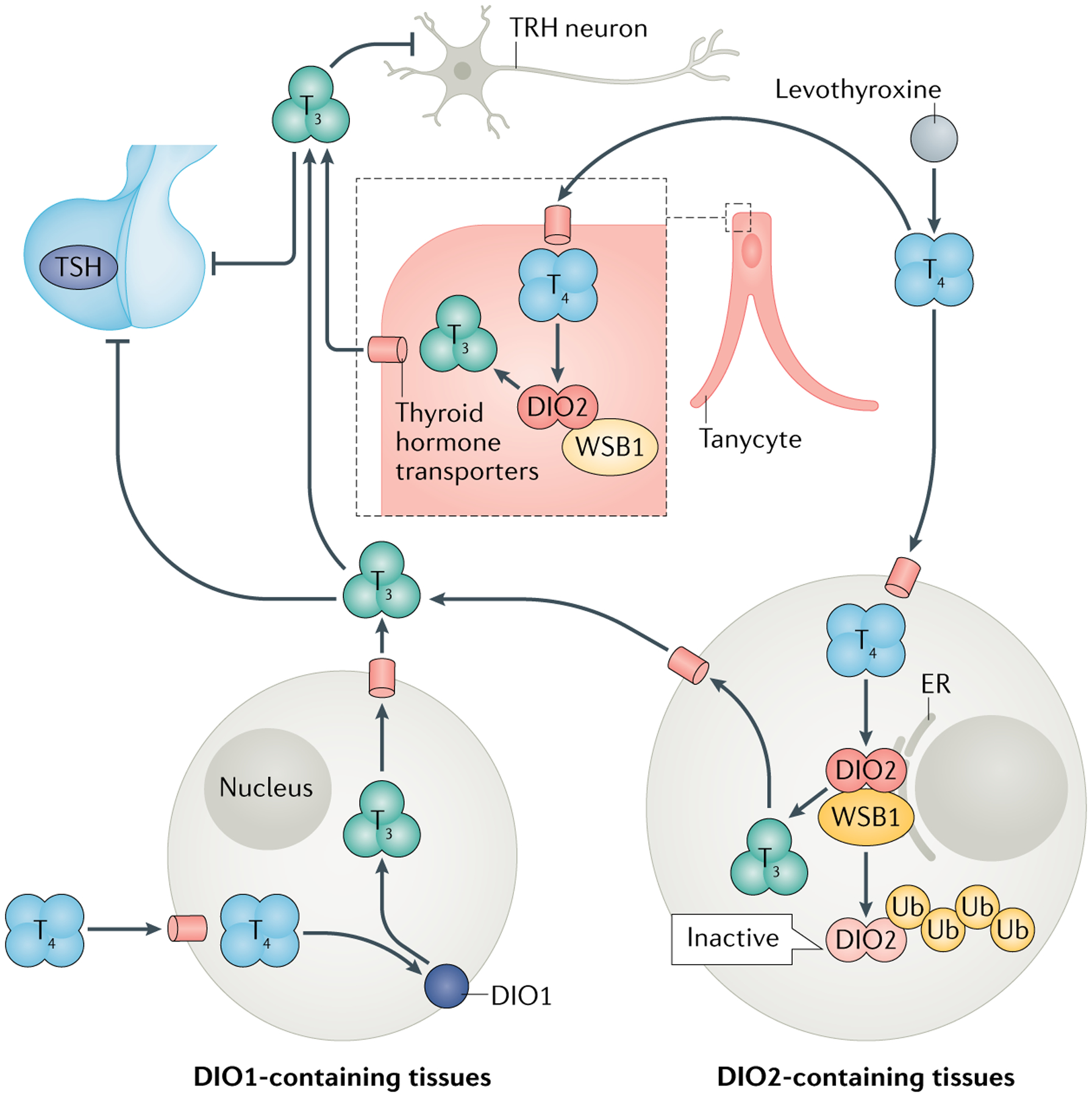
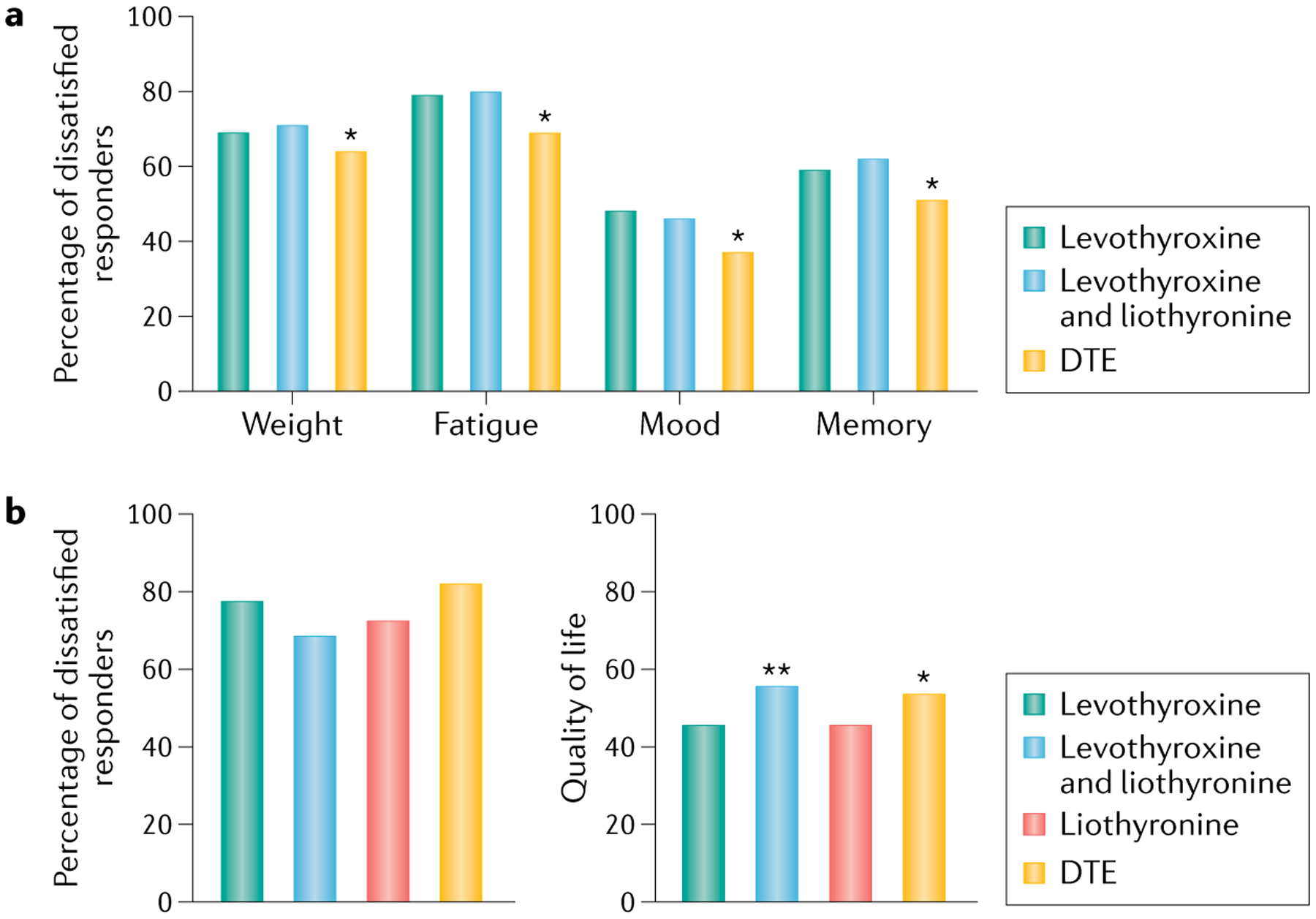
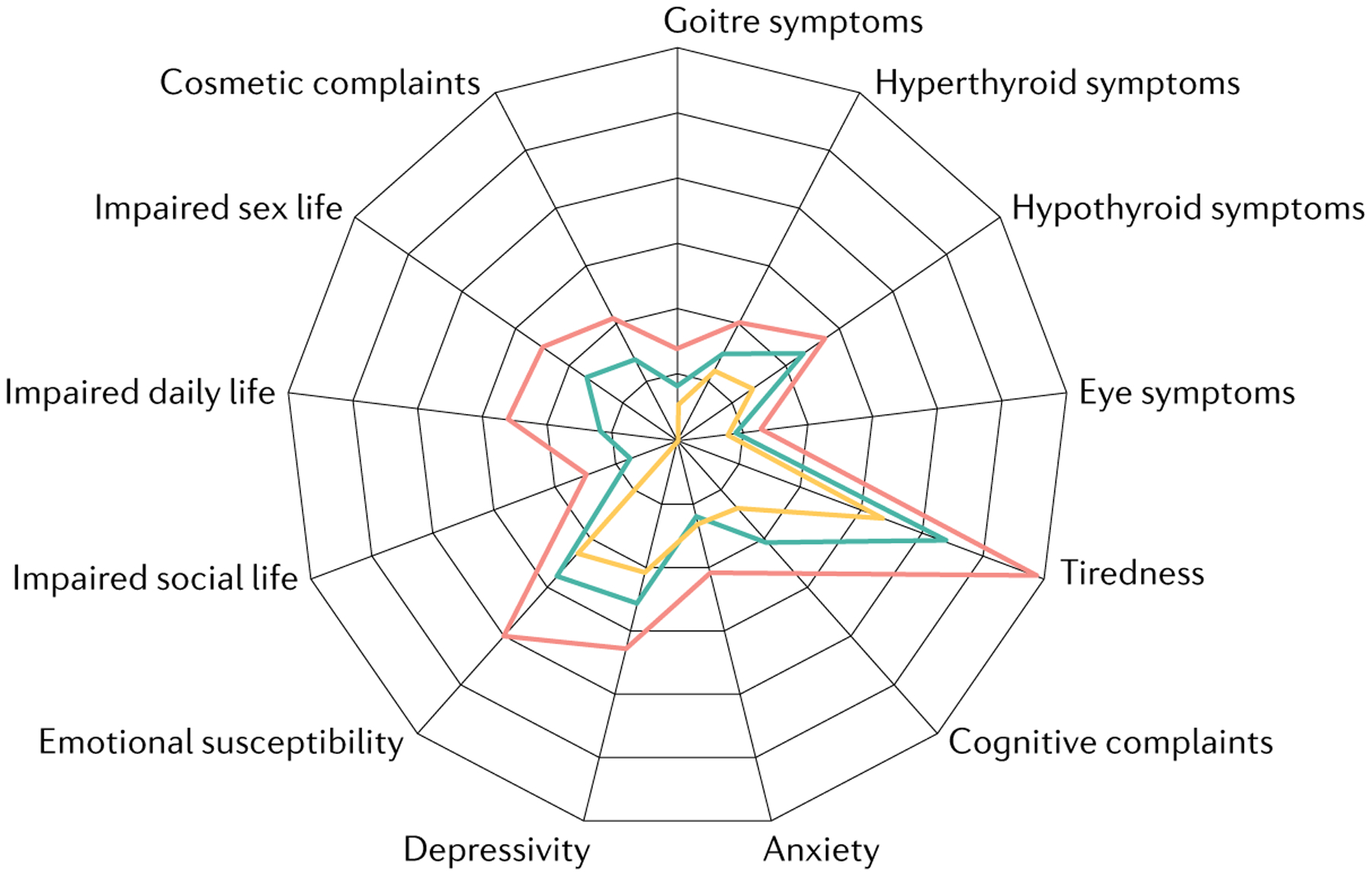
In the 1970s, treatment with thyroid extract was superseded by levothyroxine, a synthetic L form of tetraiodothyronine. Since then, no major innovation has emerged for the treatment of hypothyroidism. The biochemical definition of subclinical hypothyroidism is a matter of debate. Indiscriminate screening for hypothyroidism has led to overdiagnosis and treatment initiation at lower serum levels of thyroid-stimulating hormone (TSH) than previously. Adverse health effects have been documented in individuals with hypothyroidism or hyperthyroidism, and these adverse effects can affect health-related quality of life (QOL). Levothyroxine substitution improves, but does not always normalize, QOL, especially for individuals with mild hypothyroidism. However, neither studies combining levothyroxine and liothyronine (the synthetic form of tri-iodothyronine) nor the use of desiccated thyroid extract have shown robust improvements in patient satisfaction. Future studies should focus not only on a better understanding of an individual's TSH set point (the innate narrow physiological range of serum concentration of TSH in an individual, before the onset of hypothyroidism) and alternative thyroid hormone combinations and formulations, but also on autoimmunity and comorbidities unrelated to hypothyroidism as drivers of patient dissatisfaction. Attention to the long-term health consequences of hypothyroidism, beyond QOL, and the risks of overtreatment is imperative.
© 2022. Springer Nature Limited.
Conflict of interest statement
Competing interests
S.H.P. has received speaker fees from Quidel, Sanofi and Berlin Chemie, and consulting fees from Apitope. P.P. has received consulting fees from IBSA Institut Biochimique and speaker fees from Berlin Chemie. L.H. has received consulting fees from IBSA Institut Biochimique and speaker fees from Berlin Chemie. A.C.B. is a consultant for AbbVie, Allergan, Synthonics, Sention, and Thyron. J.J. and A.P.W. declare no competing interests.
Figures
References
-
- Okosieme O et al. Management of primary hypothyroidism: statement by the British Thyroid Association Executive Committee. Clin. Endocrinol 84, 799–808 (2016). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
