

Safety and immunogenicity of a self-amplifying RNA vaccine against COVID-19: COVAC1, a phase I, dose-ranging trial
- PMID: 35043093
- PMCID: PMC8759012
- DOI: 10.1016/j.eclinm.2021.101262
Safety and immunogenicity of a self-amplifying RNA vaccine against COVID-19: COVAC1, a phase I, dose-ranging trial
Abstract
Background: Lipid nanoparticle (LNP) encapsulated self-amplifying RNA (saRNA) is a novel technology formulated as a low dose vaccine against COVID-19.
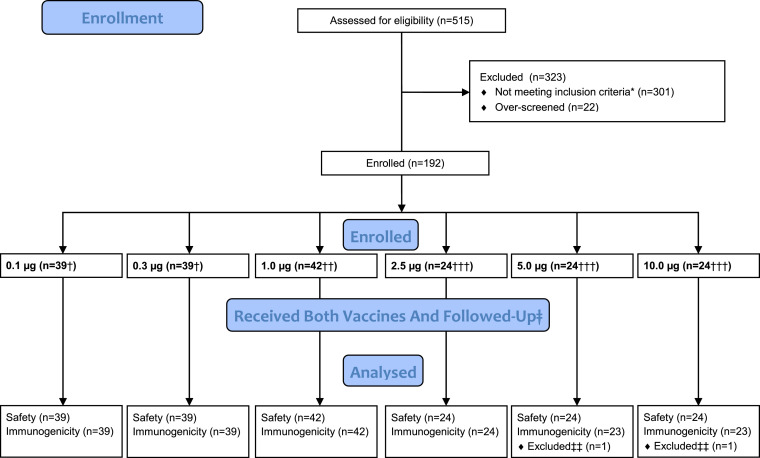
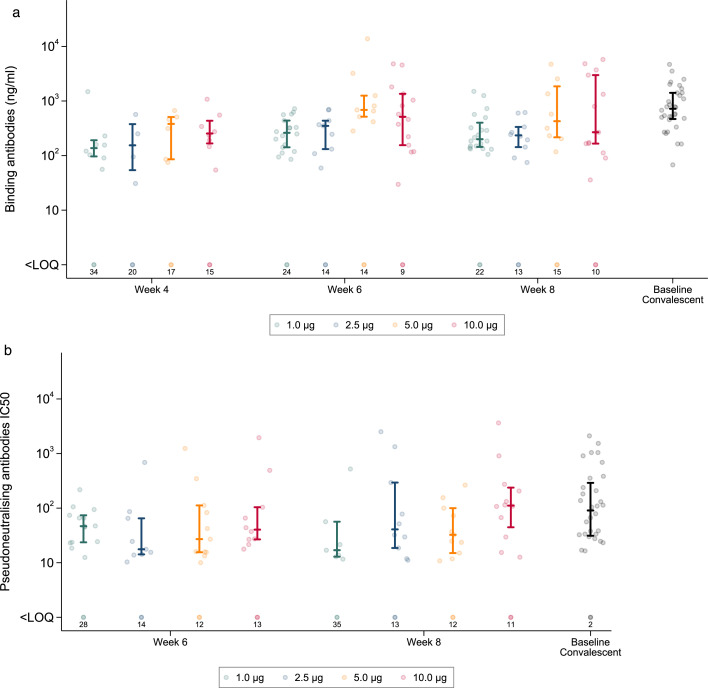
Methods: A phase I first-in-human dose-ranging trial of a saRNA COVID-19 vaccine candidate LNP-nCoVsaRNA, was conducted at Imperial Clinical Research Facility, and participating centres in London, UK, between 19th June to 28th October 2020. Participants received two intramuscular (IM) injections of LNP-nCoVsaRNA at six different dose levels, 0.1-10.0μg, given four weeks apart. An open-label dose escalation was followed by a dose evaluation. Solicited adverse events (AEs) were collected for one week from enrolment, with follow-up at regular intervals (1-8 weeks). The binding and neutralisation capacity of anti-SARS-CoV-2 antibody raised in participant sera was measured by means of an anti-Spike (S) IgG ELISA, immunoblot, SARS-CoV-2 pseudoneutralisation and wild type neutralisation assays. (The trial is registered: ISRCTN17072692, EudraCT 2020-001646-20).
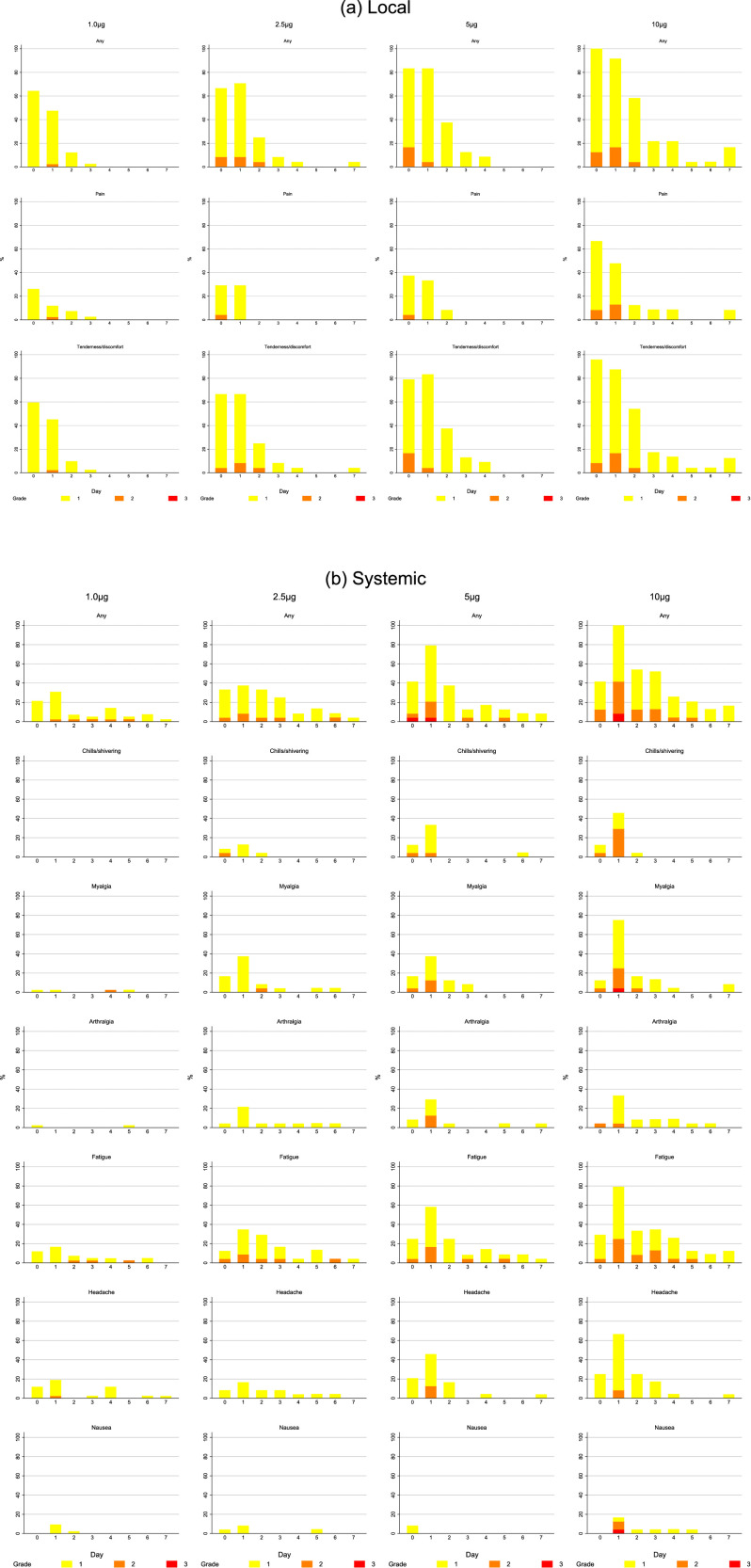
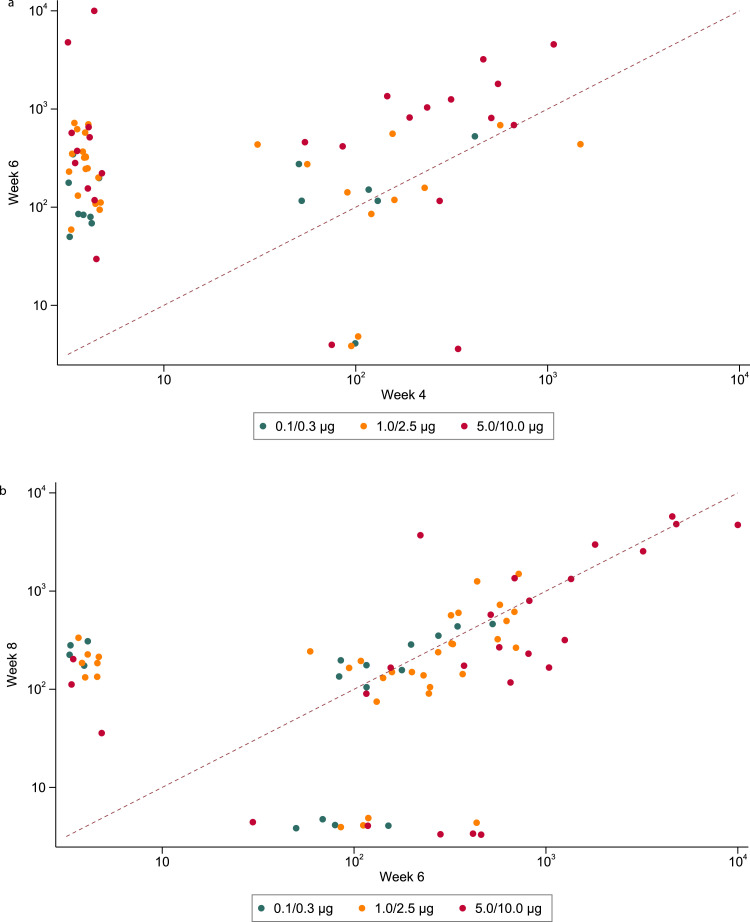
Findings: 192 healthy individuals with no history or serological evidence of COVID-19, aged 18-45 years were enrolled. The vaccine was well tolerated with no serious adverse events related to vaccination. Seroconversion at week six whether measured by ELISA or immunoblot was related to dose (both p<0.001), ranging from 8% (3/39; 0.1μg) to 61% (14/23; 10.0μg) in ELISA and 46% (18/39; 0.3μg) to 87% (20/23; 5.0μg and 10.0μg) in a post-hoc immunoblot assay. Geometric mean (GM) anti-S IgG concentrations ranged from 74 (95% CI, 45-119) at 0.1μg to 1023 (468-2236) ng/mL at 5.0μg (p<0.001) and was not higher at 10.0μg. Neutralisation of SARS-CoV-2 by participant sera was measurable in 15% (6/39; 0.1μg) to 48% (11/23; 5.0μg) depending on dose level received.
Interpretation: Encapsulated saRNA is safe for clinical development, is immunogenic at low dose levels but failed to induce 100% seroconversion. Modifications to optimise humoral responses are required to realise its potential as an effective vaccine against SARS-CoV-2.
Funding: This study was co-funded by grants and gifts from the Medical Research Council UKRI (MC_PC_19076), and the National Institute Health Research/Vaccine Task Force, Partners of Citadel and Citadel Securities, Sir Joseph Hotung Charitable Settlement, Jon Moulton Charity Trust, Pierre Andurand, Restore the Earth.
Keywords: AEs, adverse events; GOI, gene of Interest; LNP, lipid nanoparticle; NSP, non-structural protein; VEEV, Venezuelan equine encephalitis virus; saRNA, self-amplifying RNA.
© 2021 The Authors.
Conflict of interest statement
P.F.M. and R.J.S. are co-inventors on a patent application covering this SARS-CoV-2 saRNA vaccine. All the other authors have nothing to report.
Figures
References
-
- Bernstein DI, Reap EA, Katen K, et al. Randomized, double-blind, Phase 1 trial of an alphavirus replicon vaccine for cytomegalovirus in CMV seronegative adult volunteers. Vaccine. 2009;28:484–493. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
