

Clinical Predictors and Long-term Impact of Acute Kidney Injury on Progression of Diabetic Kidney Disease in Chinese Patients With Type 2 Diabetes
- PMID: 35043149
- PMCID: PMC8893937
- DOI: 10.2337/db21-0694
Clinical Predictors and Long-term Impact of Acute Kidney Injury on Progression of Diabetic Kidney Disease in Chinese Patients With Type 2 Diabetes
Abstract
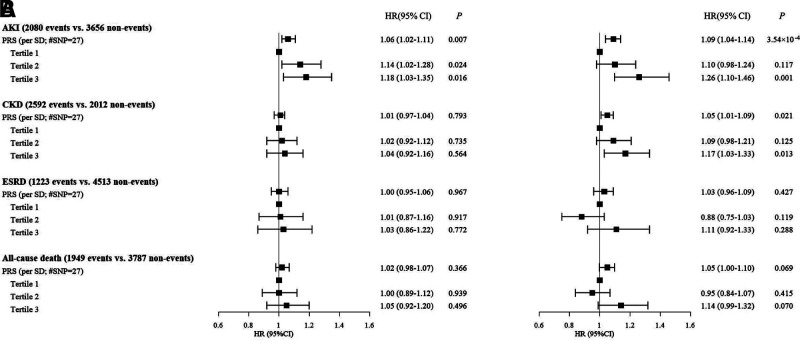
We aim to assess the long-term impact of acute kidney injury (AKI) on progression of diabetic kidney disease (DKD) and all-cause mortality and investigate determinants of AKI in Chinese patients with type 2 diabetes (T2D). A consecutive cohort of 9,096 Chinese patients with T2D from the Hong Kong Diabetes Register was followed for 12 years (mean ± SD age 57 ± 13.2 years; 46.9% men; median duration of diabetes 5 years). AKI was defined based on the Kidney Disease: Improving Global Outcomes (KDIGO) criteria using serum creatinine. Estimated glomerular filtration rate measurements were used to identify the first episode with chronic kidney disease (CKD) and end-stage renal disease (ESRD). Polygenic risk score (PRS) composed of 27 single nucleotide polymorphisms (SNPs) known to be associated with serum uric acid (SUA) in European populations was used to examine the role of SUA in pathogenesis of AKI, CKD, and ESRD. Validation was sought in an independent cohort including 6,007 patients (age 61.2 ± 10.9 years; 59.5% men; median duration of diabetes 10 years). Patients with AKI had a higher risk for developing incident CKD (hazard ratio 14.3 [95% CI 12.69-16.11]), for developing ESRD (12.1 [10.74-13.62]), and for all-cause death (7.99 [7.31-8.74]) compared with those without AKI. Incidence rate for ESRD among patients with no episodes of AKI and one, two, and three or more episodes of AKI was 7.1, 24.4, 32.4, and 37.3 per 1,000 person-years, respectively. Baseline SUA was a strong independent predictor for AKI. A PRS composed of 27 SUA-related SNPs was associated with AKI and CKD in both discovery and replication cohorts but not ESRD. Elevated SUA may increase the risk of DKD through increasing AKI. The identification of SUA as a modifiable risk factor and PRS as a nonmodifiable risk factor may facilitate the identification of individuals at high risk to prevent AKI and its long-term impact in T2D.
© 2022 by the American Diabetes Association.
Figures
References
-
- McKnight AJ, Duffy S, Maxwell AP. Genetics of diabetic nephropathy: a long road of discovery. Curr Diab Rep 2015;15:41. - PubMed
-
- Vupputuri S, Kimes TM, Calloway MO, et al. . The economic burden of progressive chronic kidney disease among patients with type 2 diabetes. J Diabetes Complications 2014;28:10–16 - PubMed
-
- Wu AYT, Kong NCT, de Leon FA, et al. . An alarmingly high prevalence of diabetic nephropathy in Asian type 2 diabetic patients: the MicroAlbuminuria Prevalence (MAP) Study. Diabetologia 2005;48:17–26 - PubMed
-
- Jha V. Current status of chronic kidney disease care in southeast Asia. Semin Nephrol 2009;29:487–496 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
