

Heterogeneity of DKA Incidence and Age-Specific Clinical Characteristics in Children Diagnosed With Type 1 Diabetes in the TEDDY Study
- PMID: 35043162
- PMCID: PMC8918232
- DOI: 10.2337/dc21-0422
Heterogeneity of DKA Incidence and Age-Specific Clinical Characteristics in Children Diagnosed With Type 1 Diabetes in the TEDDY Study
Abstract
Objective: The Environmental Determinants of Diabetes in the Young (TEDDY) study is uniquely capable of investigating age-specific differences associated with type 1 diabetes. Because age is a primary driver of heterogeneity in type 1 diabetes, we sought to characterize by age metabolic derangements prior to diagnosis and clinical features associated with diabetic ketoacidosis (DKA).
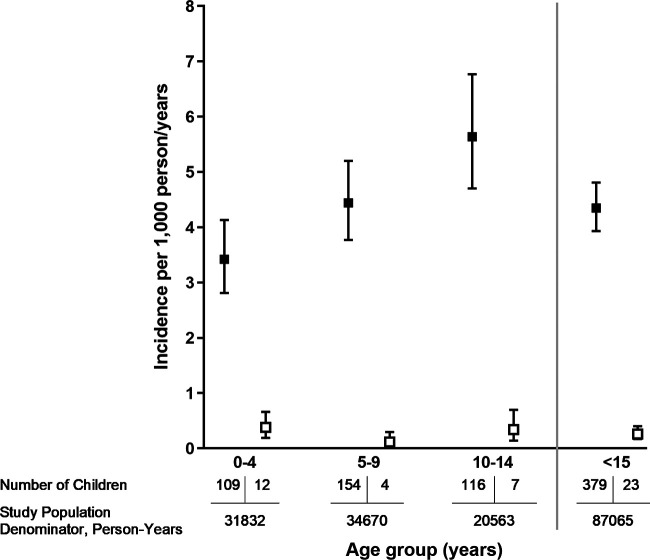
Research design and methods: The 379 TEDDY children who developed type 1 diabetes were grouped by age at onset (0-4, 5-9, and 10-14 years; n = 142, 151, and 86, respectively) with comparisons of autoantibody profiles, HLAs, family history of diabetes, presence of DKA, symptomatology at onset, and adherence to TEDDY protocol. Time-varying analysis compared those with oral glucose tolerance test data with TEDDY children who did not progress to diabetes.
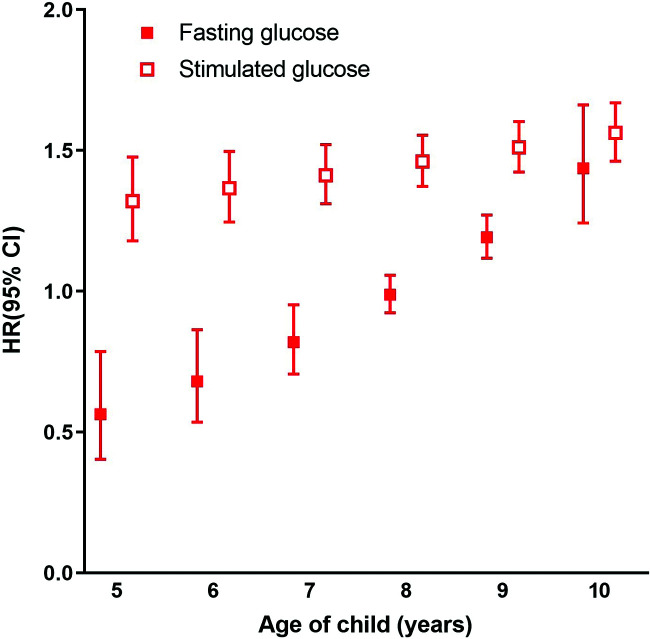
Results: Increasing fasting glucose (hazard ratio [HR] 1.09 [95% CI 1.04-1.14]; P = 0.0003), stimulated glucose (HR 1.50 [1.42-1.59]; P < 0.0001), fasting insulin (HR 0.89 [0.83-0.95]; P = 0.0009), and glucose-to-insulin ratio (HR 1.29 [1.16-1.43]; P < 0.0001) were associated with risk of progression to type 1 diabetes. Younger children had fewer autoantibodies with more symptoms at diagnosis. Twenty-three children (6.1%) had DKA at onset, only 1 (0.97%) of 103 with and 22 (8.0%) of 276 children without a first-degree relative (FDR) with type 1 diabetes (P = 0.008). Children with DKA were more likely to be nonadherent to study protocol (P = 0.047), with longer duration between their last TEDDY evaluation and diagnosis (median 10.2 vs. 2.0 months without DKA; P < 0.001).
Conclusions: DKA at onset in TEDDY is uncommon, especially for FDRs. For those without familial risk, metabolic monitoring continues to provide a primary benefit of reduced DKA but requires regular follow-up. Clinical and laboratory features vary by age at onset, adding to the heterogeneity of type 1 diabetes.
© 2022 by the American Diabetes Association.
Figures
References
-
- International Diabetes Federation . IDF Diabetes Atlas, eighth edition, 2017. Accessed 29 November 2020. Available from https://diabetesatlas.org/upload/resources/previous/files/8/IDF_DA_8e-EN...
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U01 DK063821/DK/NIDDK NIH HHS/United States
- UC4 DK063863/DK/NIDDK NIH HHS/United States
- UL1 TR002535/TR/NCATS NIH HHS/United States
- HHSN267200700014C/DK/NIDDK NIH HHS/United States
- U01 DK063790/DK/NIDDK NIH HHS/United States
- UL1 TR000064/TR/NCATS NIH HHS/United States
- U01 DK063836/DK/NIDDK NIH HHS/United States
- U01 DK063829/DK/NIDDK NIH HHS/United States
- U01 DK063865/DK/NIDDK NIH HHS/United States
- UC4 DK095300/DK/NIDDK NIH HHS/United States
- UC4 DK063861/DK/NIDDK NIH HHS/United States
- UC4 DK063829/DK/NIDDK NIH HHS/United States
- UC4 DK063821/DK/NIDDK NIH HHS/United States
- UC4 DK117483/DK/NIDDK NIH HHS/United States
- UC4 DK063836/DK/NIDDK NIH HHS/United States
- UC4 DK112243/DK/NIDDK NIH HHS/United States
- U01 DK124166/DK/NIDDK NIH HHS/United States
- U01 DK063861/DK/NIDDK NIH HHS/United States
- UC4 DK063865/DK/NIDDK NIH HHS/United States
- U01 DK063863/DK/NIDDK NIH HHS/United States
- UC4 DK106955/DK/NIDDK NIH HHS/United States
- UC4 DK100238/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
