

Comparison of Prolonged Exposure vs Cognitive Processing Therapy for Treatment of Posttraumatic Stress Disorder Among US Veterans: A Randomized Clinical Trial
- PMID: 35044471
- PMCID: PMC8771295
- DOI: 10.1001/jamanetworkopen.2021.36921
Comparison of Prolonged Exposure vs Cognitive Processing Therapy for Treatment of Posttraumatic Stress Disorder Among US Veterans: A Randomized Clinical Trial
Abstract
Importance: Posttraumatic stress disorder (PTSD) is a prevalent and serious mental health problem. Although there are effective psychotherapies for PTSD, there is little information about their comparative effectiveness.
Objective: To compare the effectiveness of prolonged exposure (PE) vs cognitive processing therapy (CPT) for treating PTSD in veterans.
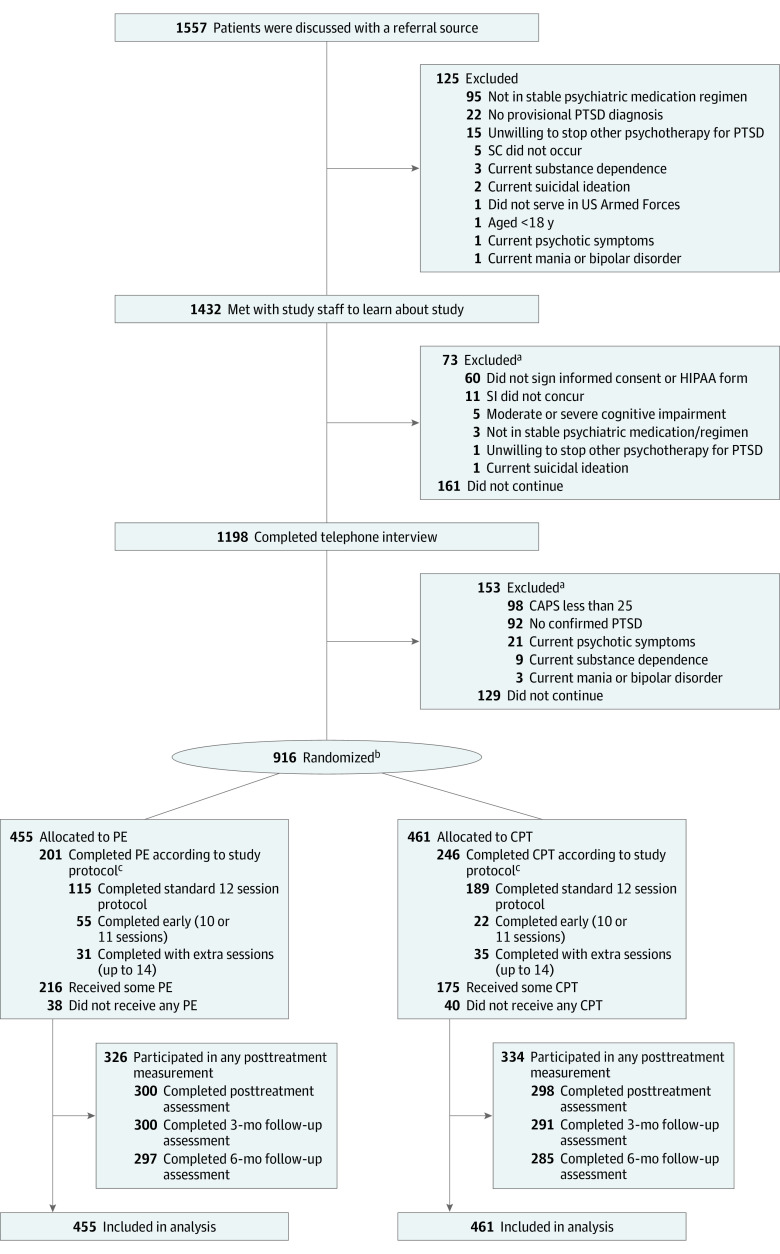
Design, setting, and participants: This randomized clinical trial assessed the comparative effectiveness of PE vs CPT among veterans with military-related PTSD recruited from outpatient mental health clinics at 17 Department of Veterans Affairs medical centers across the US from October 31, 2014, to February 1, 2018, with follow-up through February 1, 2019. The primary outcome was assessed using centralized masking. Tested hypotheses were prespecified before trial initiation. Data were analyzed from October 5, 2020, to May 5, 2021.
Interventions: Participants were randomized to 1 of 2 individual cognitive-behavioral therapies, PE or CPT, delivered according to a flexible protocol of 10 to 14 sessions.
Main outcomes and measures: The primary outcome was change in PTSD symptom severity on the Clinician-Administered PTSD Scale for DSM-5 (CAPS-5) from before treatment to the mean after treatment across posttreatment and 3- and 6-month follow-ups. Secondary outcomes included other symptoms, functioning, and quality of life.
Results: Analyses were based on all 916 randomized participants (730 [79.7%] men and 186 [20.3%] women; mean [range] age 45.2 [21-80] years), with 455 participants randomized to PE (mean CAPS-5 score at baseline, 39.9 [95% CI, 39.1-40.7] points) and 461 participants randomized to CPT (mean CAPS-5 score at baseline, 40.3 [95% CI, 39.5-41.1] points). PTSD severity on the CAPS-5 improved substantially in both PE (standardized mean difference [SMD], 0.99 [95% CI, 0.89-1.08]) and CPT (SMD, 0.71 [95% CI, 0.61-0.80]) groups from before to after treatment. Mean improvement was greater in PE than CPT (least square mean, 2.42 [95% CI, 0.53-4.31]; P = .01), but the difference was not clinically significant (SMD, 0.17). Results for self-reported PTSD symptoms were comparable with CAPS-5 findings. The PE group had higher odds of response (odds ratio [OR], 1.32 [95% CI, 1.00-1.65]; P < .001), loss of diagnosis (OR, 1.43 [95% CI, 1.12-1.74]; P < .001), and remission (OR, 1.62 [95% CI, 1.24-2.00]; P < .001) compared with the CPT group. Groups did not differ on other outcomes. Treatment dropout was higher in PE (254 participants [55.8%]) than in CPT (215 participants [46.6%]; P < .01). Three participants in the PE group and 1 participant in the CPT group were withdrawn from treatment, and 3 participants in each treatment dropped out owing to serious adverse events.
Conclusions and relevance: This randomized clinical trial found that although PE was statistically more effective than CPT, the difference was not clinically significant, and improvements in PTSD were meaningful in both treatment groups. These findings highlight the importance of shared decision-making to help patients understand the evidence and select their preferred treatment.
Trial registration: ClinicalTrials.gov Identifier: NCT01928732.
Conflict of interest statement
Figures
References
-
- The Management of Posttraumatic Stress Disorder Work Group . VA/DoD Clinical Practice Guideline for the Management of Posttraumatic Stress Disorder and Acute Stress Disorder, Version 3.0. Department of Veterans Affairs and Department of Defense; 2017.
-
- American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Association; 2013.
-
- Goldstein RB, Smith SM, Chou SP, et al. . The epidemiology of DSM-5 posttraumatic stress disorder in the United States: results from the National Epidemiologic Survey on Alcohol and Related Conditions-III. Soc Psychiatry Psychiatr Epidemiol. 2016;51(8):1137-1148. doi:10.1007/s00127-016-1208-5 - DOI - PMC - PubMed
