

COVID-19-mediated patient delay caused increased total ischaemic time in ST-segment elevation myocardial infarction
- PMID: 35044627
- PMCID: PMC8767528
- DOI: 10.1007/s12471-021-01653-9
COVID-19-mediated patient delay caused increased total ischaemic time in ST-segment elevation myocardial infarction
Abstract
Background: The current study aimed to evaluate changes in treatment delay and outcome for ST-segment elevation myocardial infarction (STEMI) in the Netherlands during the first coronavirus disease 2019 (COVID-19) outbreak, thereby comparing regions with a high and low COVID-19 hospitalisation rate.
Methods: Clinical characteristics, STEMI timing variables, 30-day all-cause mortality and cardiovascular complications of all consecutive patients admitted for STEMI from 1 January to 30 June in 2020 and 2019 to six hospitals performing a high volume of percutaneous coronary interventions were collected retrospectively using data from the Netherlands Heart Registry, hospital records and ambulance report forms. Patient delay, pre-hospital delay and door-to-balloon time before and after the outbreak of COVID-19 were compared to the equivalent periods in 2019.
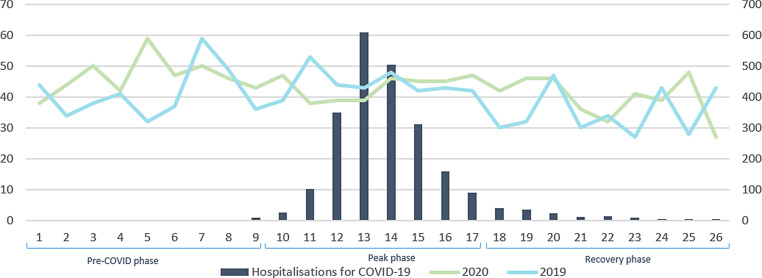
Results: A total of 2169 patients were included. During the outbreak median total treatment delay significantly increased (2 h 51 min vs 2 h 32 min; p = 0.043) due to an increased patient delay (1 h 20 min vs 1 h; p = 0.030) with more late presentations > 24 h (1.1% vs 0.3%) in 2020. This increase was particularly evident during the peak phase of COVID-19 in regions with a high COVID-19 hospitalisation rate. During the peak phase door-to-balloon time was shorter (38 min vs 43 min; p = 0.042) than in 2019. All-cause 30-day mortality was comparable in both time frames (7.8% vs 7.3%; p = 0.797).
Conclusions: During the outbreak of COVID-19 patient delay caused an increase in total ischaemic time for STEMI, with a more pronounced delay in high-endemic regions, stressing the importance of good patient education during comparable crisis situations.
Keywords: COVID-19; Door-to-balloon time; Percutaneous coronary intervention; ST-segment myocardial infarction; Treatment delay.
© 2022. The Author(s).
Conflict of interest statement
H. N. Sturkenboom, V. A. E. van Hattem, W. Nieuwland, F. M. A. Paris, M. Magro, R. L. Anthonio, A. Algin, E. Lipsic, E. Bruwiere, B. J. L. Van den Branden, J. Polad, P. Tonino and R. A. Tio declare that they have no competing interests.
Figures

References
-
- Scholz KH, Maier SKG, Maier LS, et al. Impact of treatment delay on mortality in ST-segment elevation myocardial infarction (STEMI) patients presenting with and without haemodynamic instability: results from the German prospective, multicentre FITT-STEMI trial. Eur Heart J. 2018;39:1065–1074. doi: 10.1093/eurheartj/ehy004. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
