

Cost-Effectiveness of Coronary Artery Bypass Surgery Versus Medicine in Ischemic Cardiomyopathy: The STICH Randomized Clinical Trial
- PMID: 35044802
- PMCID: PMC8959089
- DOI: 10.1161/CIRCULATIONAHA.121.056276
Cost-Effectiveness of Coronary Artery Bypass Surgery Versus Medicine in Ischemic Cardiomyopathy: The STICH Randomized Clinical Trial
Abstract
Background: The STICH Randomized Clinical Trial (Surgical Treatment for Ischemic Heart Failure) demonstrated that coronary artery bypass grafting (CABG) reduced all-cause mortality rates out to 10 years compared with medical therapy alone (MED) in patients with ischemic cardiomyopathy and reduced left ventricular function (ejection fraction ≤35%). We examined the economic implications of these results.
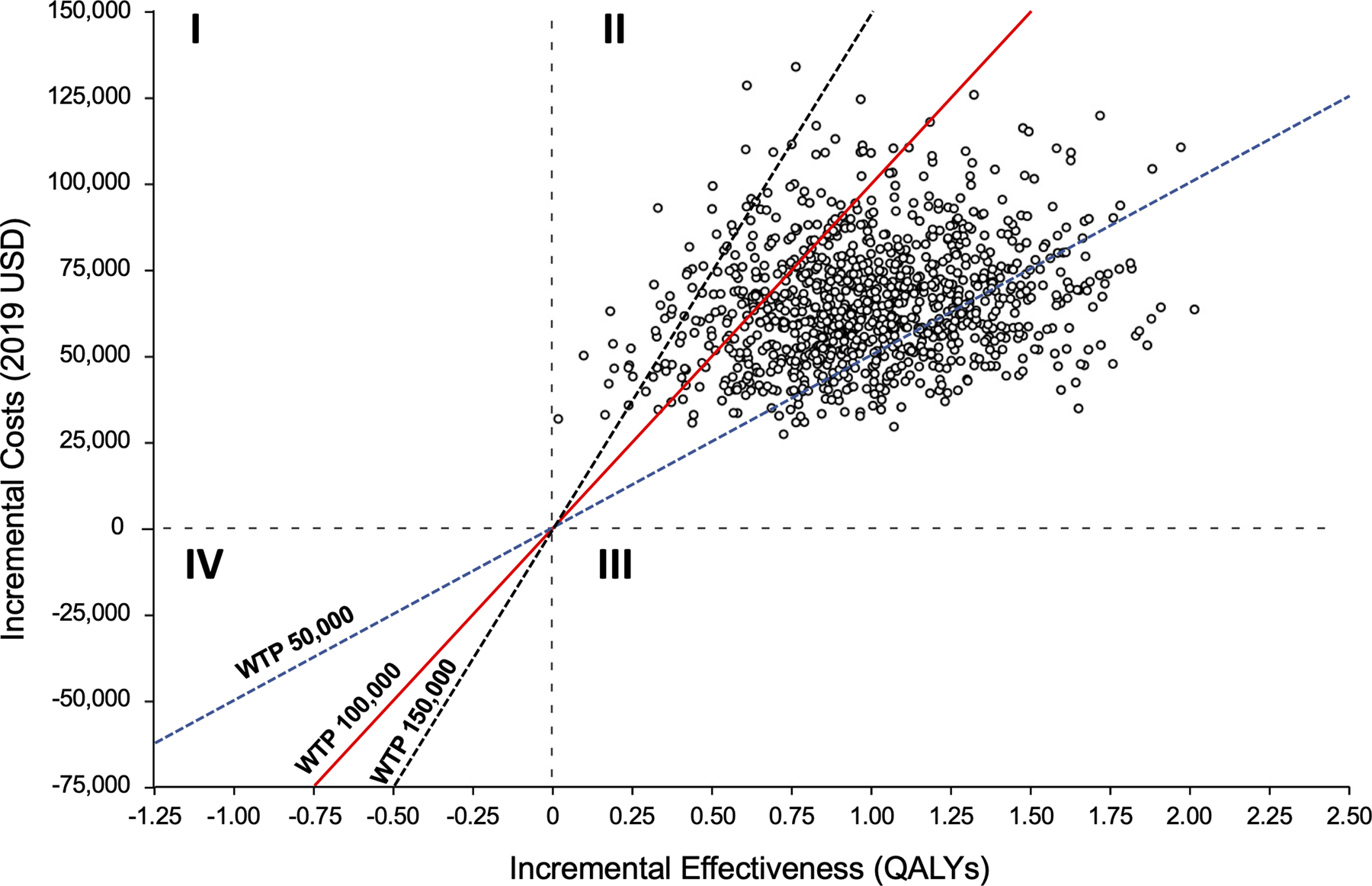
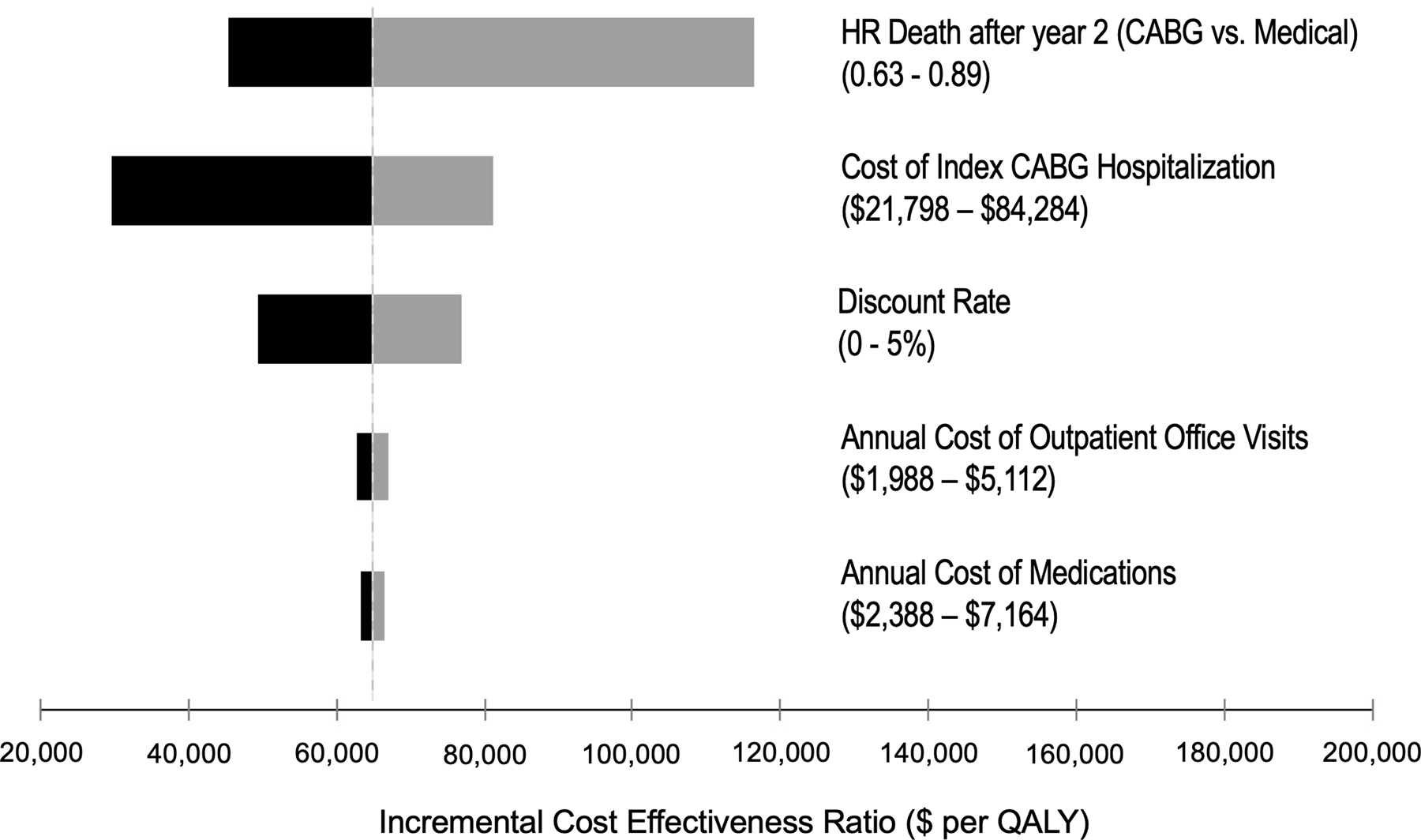
Methods: We used a decision-analytic patient-level simulation model to estimate the lifetime costs and benefits of CABG and MED using patient-level resource use and clinical data collected in the STICH trial. Patient-level costs were calculated by applying externally derived US cost weights to resource use counts during trial follow-up. A 3% discount rate was applied to both future costs and benefits. The primary outcome was the incremental cost-effectiveness ratio assessed from the US health care sector perspective.
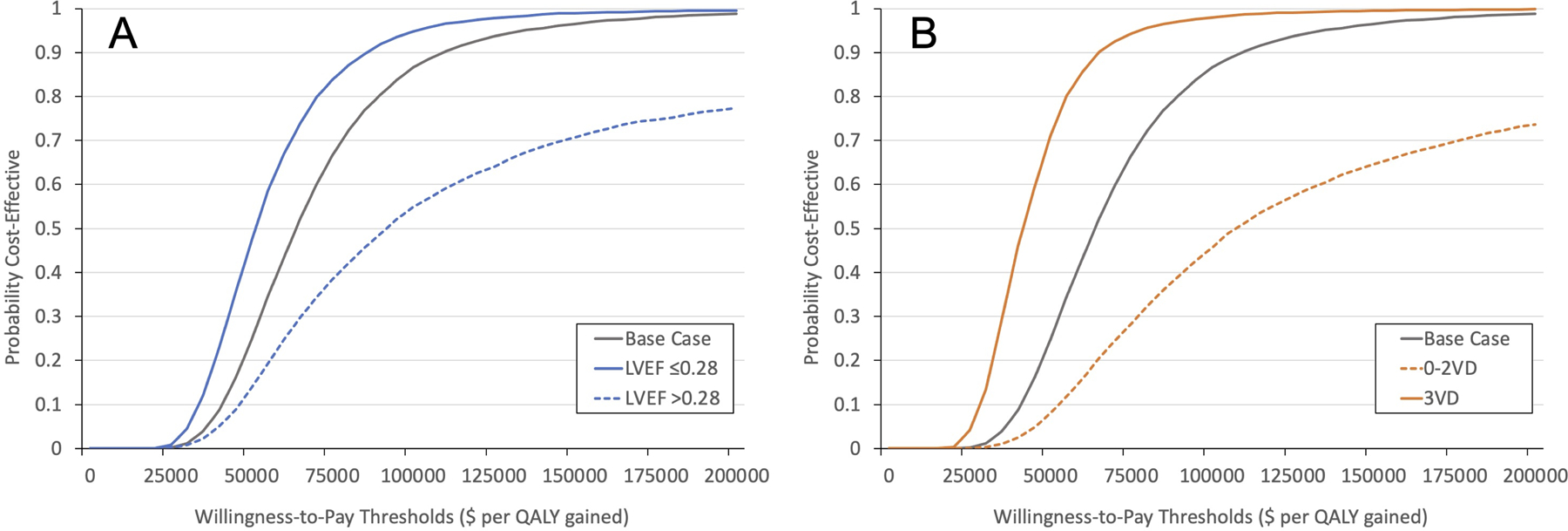
Results: For the CABG arm, we estimated 6.53 quality-adjusted life-years (95% CI, 5.70-7.53) and a lifetime cost of $140 059 (95% CI, $106 401 to $180 992). For the MED arm, the corresponding estimates were 5.52 (95% CI, 5.06-6.09) quality-adjusted life-years and $74 894 lifetime cost (95% CI, $58 372 to $93 541). The incremental cost-effectiveness ratio for CABG compared with MED was $63 989 per quality-adjusted life-year gained. At a societal willingness-to-pay threshold of $100 000 per quality-adjusted life-year gained, CABG was found to be economically favorable compared with MED in 87% of microsimulations.
Conclusions: In the STICH trial, in patients with ischemic cardiomyopathy and reduced left ventricular function, CABG was economically attractive relative to MED at current benchmarks for value in the United States.
Registration: URL: https://www.
Clinicaltrials: gov; Unique identifier: NCT00023595.
Keywords: cardiomyopathies; coronary artery bypass; coronary artery disease; cost-benefit analysis; costs and cost analysis.
Figures
References
-
- Balmforth C, Simpson J, Shen L, Jhund PS, Lefkowitz M, Rizkala AR, Rouleau JL, Shi V, Solomon SD, Swedberg K, Zile MR, Packer M and McMurray JJV. Outcomes and Effect of Treatment According to Etiology in HFrEF: An Analysis of PARADIGM-HF. JACC Heart Fail. 2019;7:457–465. - PubMed
-
- Virani SS, Alonso A, Aparicio HJ, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Cheng S, et al., American Heart Association Council on Epidemiology, Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2021 Update: A Report From the American Heart Association. Circulation. 2021;143:e254–e743. - PubMed
-
- Murphy SP, Ibrahim NE and Januzzi JL. Heart failure with reduced ejection fraction: a review. JAMA. 2020;324:488–504. - PubMed
-
- Braunwald E and Rutherford JD. Reversible ischemic left ventricular dysfunction: evidence for the “hibernating myocardium”. J Am Coll Cardiol. 1986;8:1467–1470. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
