

Brief Digital Interventions to Support the Psychological Well-being of NHS Staff During the COVID-19 Pandemic: 3-Arm Pilot Randomized Controlled Trial
- PMID: 35044927
- PMCID: PMC8982650
- DOI: 10.2196/34002
Brief Digital Interventions to Support the Psychological Well-being of NHS Staff During the COVID-19 Pandemic: 3-Arm Pilot Randomized Controlled Trial
Abstract
Background: Health and social care staff are at high risk of experiencing adverse mental health (MH) outcomes during the COVID-19 pandemic. Hence, there is a need to prioritize and identify ways to effectively support their psychological well-being (PWB). Compared to traditional psychological interventions, digital psychological interventions are cost-effective treatment options that allow for large-scale dissemination and transcend social distancing, overcome rurality, and minimize clinician time.
Objective: This study reports MH outcomes of a Consolidated Standards of Reporting Trials (CONSORT)-compliant parallel-arm pilot randomized controlled trial (RCT) examining the potential usefulness of an existing and a novel digital psychological intervention aimed at supporting psychological health among National Health Service (NHS) staff working through the COVID-19 pandemic.
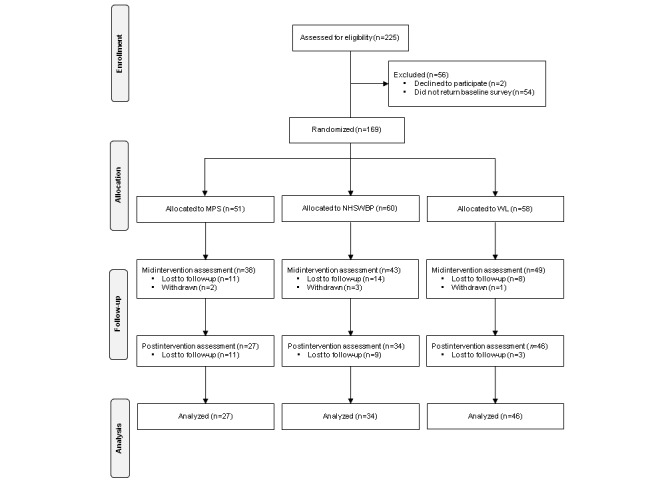
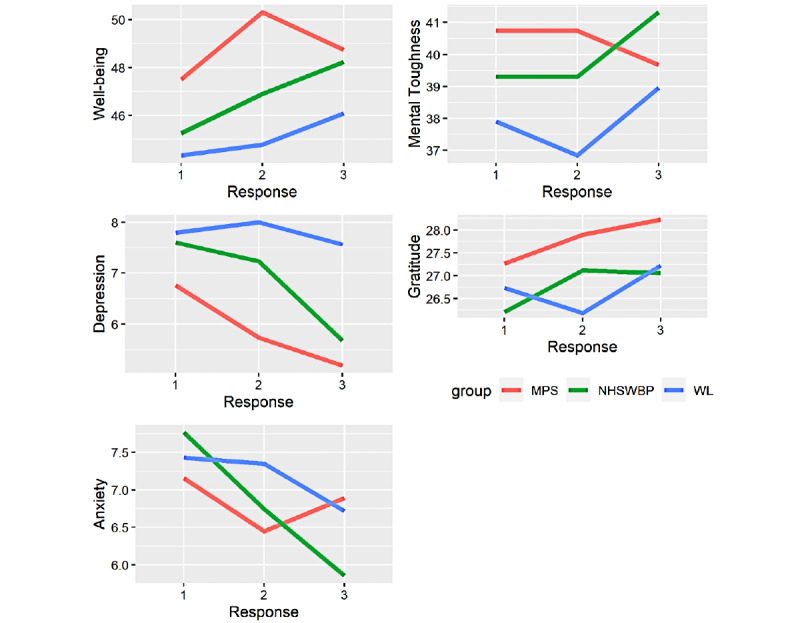
Methods: NHS Highland (NHSH) frontline staff volunteers (N=169) were randomly assigned to the newly developed NHSH Staff Wellbeing Project (NHSWBP), an established digital intervention (My Possible Self [MPS]), or a waitlist (WL) group for 4 weeks. Attempts were made to blind participants to which digital intervention they were allocated. The interventions were fully automated, without any human input or guidance. We measured 5 self-reported psychological outcomes over 3 time points: before (baseline), in the middle of (after 2 weeks), and after treatment (4 weeks). The primary outcomes were anxiety (7-item General Anxiety Disorder), depression (Patient Health Questionnaire), and mental well-being (Warwick-Edinburgh Mental Well-being Scale). The secondary outcomes included mental toughness (Mental Toughness Index) and gratitude (Gratitude Questionnaire-6).
Results: Retention rates mid- and postintervention were 77% (n=130) and 63.3% (n=107), respectively. Postintervention, small differences were noted between the WL and the 2 treatment groups on anxiety (vs MPS: Cohen d=0.07, 95% CI -0.20 to 0.33; vs NHSWBP: Cohen d=0.06, 95% CI -0.19 to 0.31), depression (vs MPS: Cohen d=0.37, 95% CI 0.07-0.66; vs NHSWBP: Cohen d=0.18, 95% CI -0.11 to 0.46), and mental well-being (vs MPS: Cohen d=-0.04, 95% CI -0.62 to -0.08; vs NHSWBP: Cohen d=-0.15, 95% CI -0.41 to 0.10). A similar pattern of between-group differences was found for the secondary outcomes. The NHSWBP group generally had larger within-group effects than the other groups and displayed a greater rate of change compared to the other groups on all outcomes, except for gratitude, where the rate of change was greatest for the MPS group.
Conclusions: Our analyses provided encouraging results for the use of brief digital psychological interventions in improving PWB among health and social care workers. Future multisite RCTs, with power to reliably detect differences, are needed to determine the efficacy of contextualized interventions relative to existing digital treatments.
Trial registration: ISRCTN Registry (ISRCTN) ISRCTN18107122; https://www.isrctn.com/ISRCTN18107122.
Keywords: COVID-19; NHS; anxiety; depression; eHealth; intervention; intervention studies; mobile health; occupational health; public health; randomized controlled trial; staff; support; well-being.
©Johannes H De Kock, Helen Ann Latham, Richard G Cowden, Breda Cullen, Katia Narzisi, Shaun Jerdan, Sarah-Anne Munoz, Stephen J Leslie, Andreas Stamatis, Jude Eze. Originally published in JMIR Mental Health (https://mental.jmir.org), 04.04.2022.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Daly M, Robinson E. Longitudinal changes in psychological distress in the UK from 2019 to September 2020 during the COVID-19 pandemic: Evidence from a large nationally representative study. Psychiatry Res. 2021 Jun;300:113920. doi: 10.1016/j.psychres.2021.113920. https://linkinghub.elsevier.com/retrieve/pii/S0165-1781(21)00217-1 S0165-1781(21)00217-1 - DOI - PMC - PubMed
-
- Petrie K, Crawford J, Baker STE, Dean K, Robinson J, Veness BG, Randall J, McGorry P, Christensen H, Harvey SB. Interventions to reduce symptoms of common mental disorders and suicidal ideation in physicians: a systematic review and meta-analysis. Lancet Psychiatry. 2019 Mar;6(3):225–234. doi: 10.1016/s2215-0366(18)30509-1. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
