Cognitive composites for genetic frontotemporal dementia: GENFI-Cog
- PMID: 35045872
- PMCID: PMC8772227
- DOI: 10.1186/s13195-022-00958-0
Cognitive composites for genetic frontotemporal dementia: GENFI-Cog
Abstract
Background: Clinical endpoints for upcoming therapeutic trials in frontotemporal dementia (FTD) are increasingly urgent. Cognitive composite scores are often used as endpoints but are lacking in genetic FTD. We aimed to create cognitive composite scores for genetic frontotemporal dementia (FTD) as well as recommendations for recruitment and duration in clinical trial design.
Methods: A standardized neuropsychological test battery covering six cognitive domains was completed by 69 C9orf72, 41 GRN, and 28 MAPT mutation carriers with CDR® plus NACC-FTLD ≥ 0.5 and 275 controls. Logistic regression was used to identify the combination of tests that distinguished best between each mutation carrier group and controls. The composite scores were calculated from the weighted averages of test scores in the models based on the regression coefficients. Sample size estimates were calculated for individual cognitive tests and composites in a theoretical trial aimed at preventing progression from a prodromal stage (CDR® plus NACC-FTLD 0.5) to a fully symptomatic stage (CDR® plus NACC-FTLD ≥ 1). Time-to-event analysis was performed to determine how quickly mutation carriers progressed from CDR® plus NACC-FTLD = 0.5 to ≥ 1 (and therefore how long a trial would need to be).
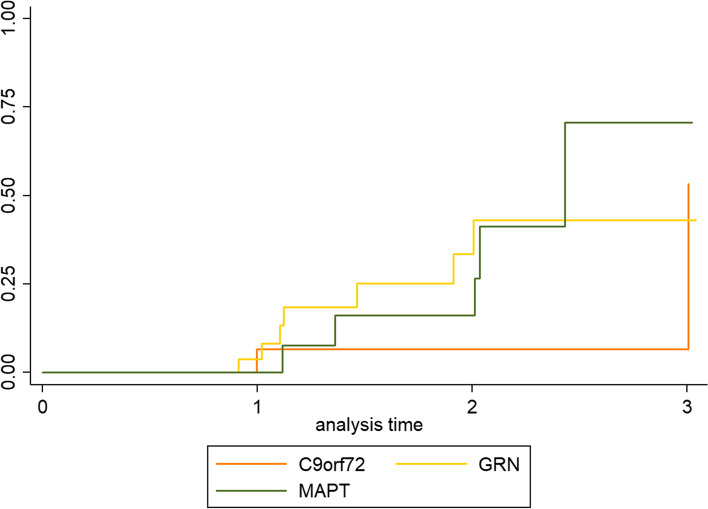
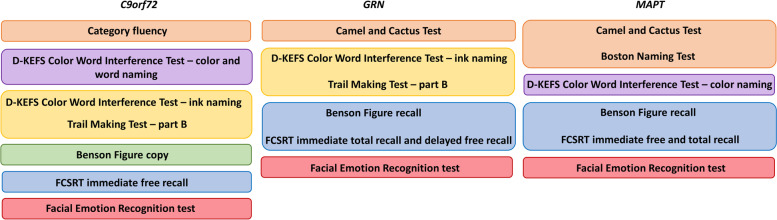
Results: The results from the logistic regression analyses resulted in different composite scores for each mutation carrier group (i.e. C9orf72, GRN, and MAPT). The estimated sample size to detect a treatment effect was lower for composite scores than for most individual tests. A Kaplan-Meier curve showed that after 3 years, ~ 50% of individuals had converted from CDR® plus NACC-FTLD 0.5 to ≥ 1, which means that the estimated effect size needs to be halved in sample size calculations as only half of the mutation carriers would be expected to progress from CDR® plus NACC FTLD 0.5 to ≥ 1 without treatment over that time period.
Discussion: We created gene-specific cognitive composite scores for C9orf72, GRN, and MAPT mutation carriers, which resulted in substantially lower estimated sample sizes to detect a treatment effect than the individual cognitive tests. The GENFI-Cog composites have potential as cognitive endpoints for upcoming clinical trials. The results from this study provide recommendations for estimating sample size and trial duration.
Keywords: Attention; Cognition; Composite score; Executive function; Frontotemporal dementia; Language; Memory; Neuropsychology; Social cognition.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures