

The QChip1 knowledgebase and microarray for precision medicine in Qatar
- PMID: 35046417
- PMCID: PMC8770564
- DOI: 10.1038/s41525-021-00270-0
The QChip1 knowledgebase and microarray for precision medicine in Qatar
Abstract
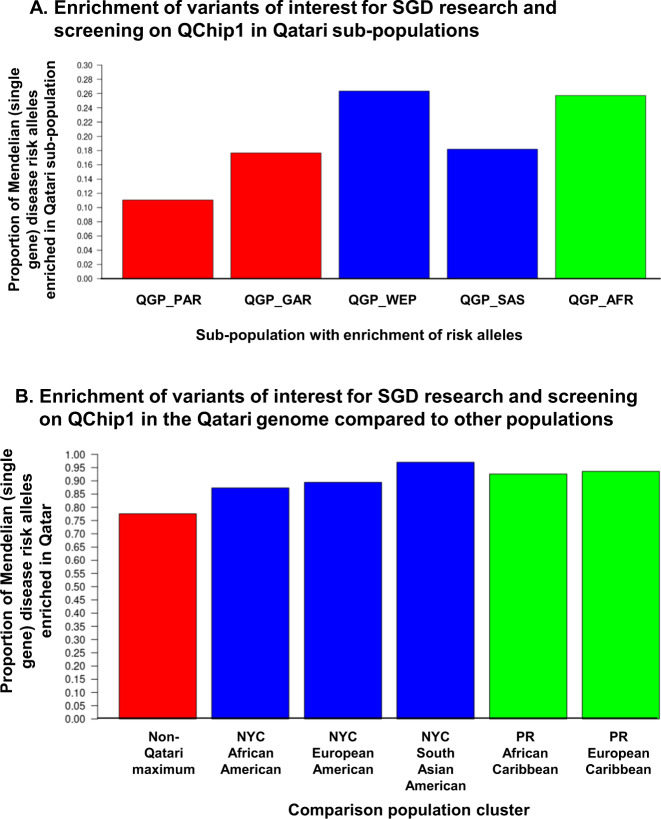
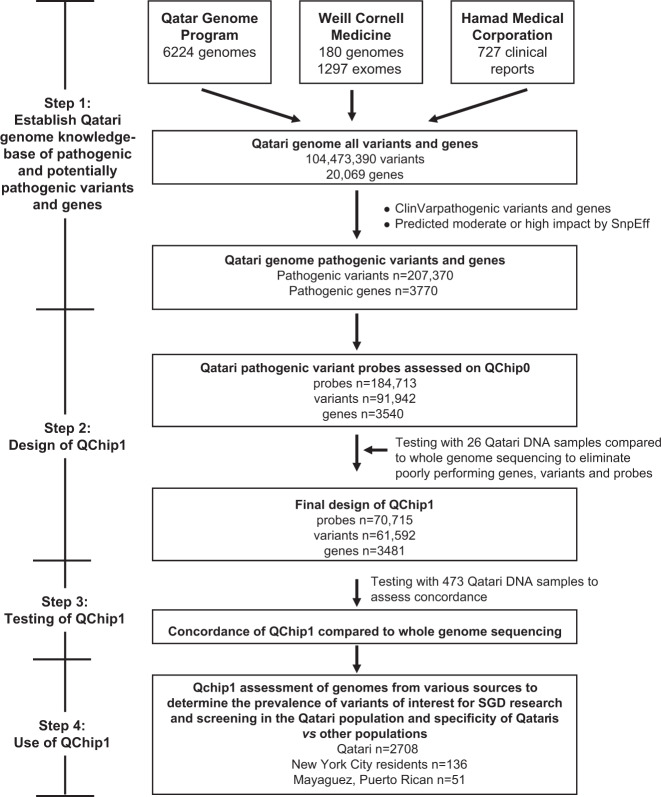
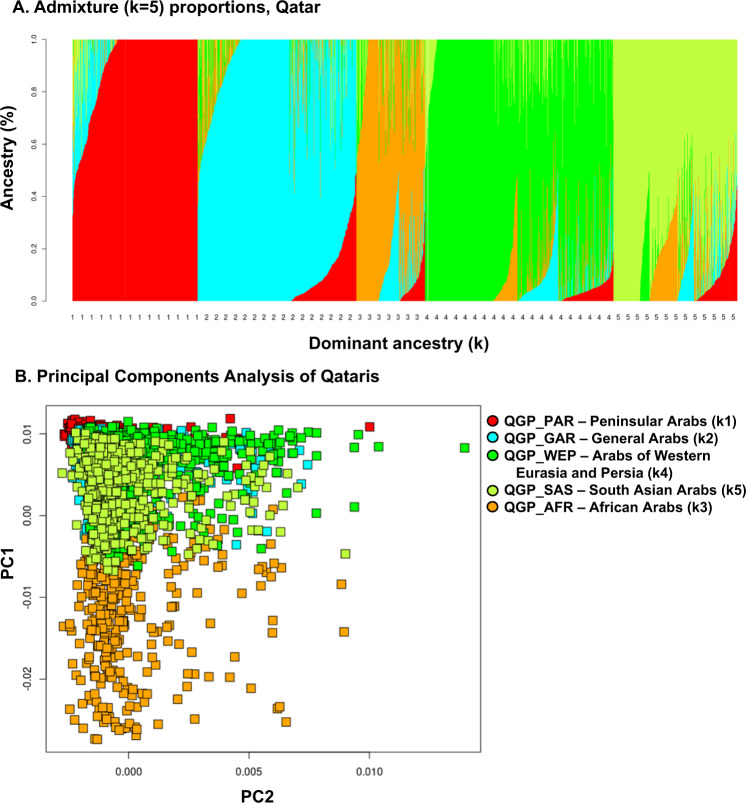
Risk genes for Mendelian (single-gene) disorders (SGDs) are consistent across populations, but pathogenic risk variants that cause SGDs are typically population-private. The goal was to develop "QChip1," an inexpensive genotyping microarray to comprehensively screen newborns, couples, and patients for SGD risk variants in Qatar, a small nation on the Arabian Peninsula with a high degree of consanguinity. Over 108 variants in 8445 Qatari were identified for inclusion in a genotyping array containing 165,695 probes for 83,542 known and potentially pathogenic variants in 3438 SGDs. QChip1 had a concordance with whole-genome sequencing of 99.1%. Testing of QChip1 with 2707 Qatari genomes identified 32,674 risk variants, an average of 134 pathogenic alleles per Qatari genome. The most common pathogenic variants were those causing homocystinuria (1.12% risk allele frequency), and Stargardt disease (2.07%). The majority (85%) of Qatari SGD pathogenic variants were not present in Western populations such as European American, South Asian American, and African American in New York City and European and Afro-Caribbean in Puerto Rico; and only 50% were observed in a broad collection of data across the Greater Middle East including Kuwait, Iran, and United Arab Emirates. This study demonstrates the feasibility of developing accurate screening tools to identify SGD risk variants in understudied populations, and the need for ancestry-specific SGD screening tools.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
