

Impact of regular additional endobiliary radiofrequency ablation on survival of patients with advanced extrahepatic cholangiocarcinoma under systemic chemotherapy
- PMID: 35046437
- PMCID: PMC8770452
- DOI: 10.1038/s41598-021-04297-2
Impact of regular additional endobiliary radiofrequency ablation on survival of patients with advanced extrahepatic cholangiocarcinoma under systemic chemotherapy
Abstract
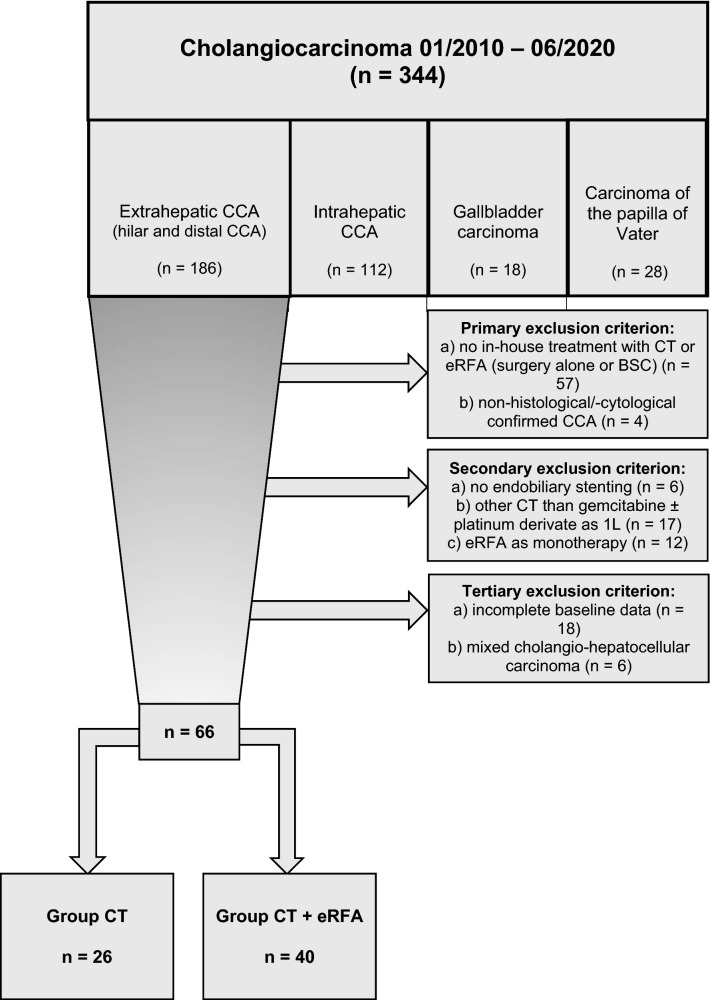
Prognosis of patients with advanced extrahepatic cholangiocarcinoma (eCCA) is poor. The current standard first-line treatment is systemic chemotherapy (CT) with gemcitabine and a platinum derivate. Additionally, endobiliary radiofrequency ablation (eRFA) can be applied to treat biliary obstructions. This study aimed to evaluate the additional benefit of scheduled regular eRFA in a real-life patient cohort with advanced extrahepatic cholangiocarcinoma under standard systemic CT. All patients with irresectable eCCA treated at University Hospital Bonn between 2010 and 2020 were eligible for inclusion. Patients were stratified according to treatment: standard CT (n = 26) vs. combination of eRFA with standard CT (n = 40). Overall survival (OS), progression free survival (PFS), feasibility and toxicity were retrospectively analyzed using univariate and multivariate approaches. Combined eRFA and CT resulted in significantly longer median OS (17.3 vs. 8.6 months, p = 0.004) and PFS (12.9 vs. 5.7 months, p = 0.045) compared to the CT only group. While groups did not differ regarding age, sex, tumor stage and chemotherapy treatment regimen, mean MELD was even higher (10.1 vs. 6.7, p = 0.015) in the eRFA + CT group. The survival benefit of concomitant eRFA was more evident in the subgroup with locally advanced tumors. Severe hematological toxicities (CTCAE grades 3 - 5) did not differ significantly between the groups. However, therapy-related cholangitis occurred more often in the combined treatment group (p = 0.031). Combination of eRFA and systemic CT was feasible, well-tolerated and could significantly prolong survival compared to standard CT alone. Thus, eRFA should be considered during therapeutic decision making in advanced eCCA.
© 2022. The Author(s).
Conflict of interest statement
Author T.W. has received speaker fees from Boston Scientific, Cook-Medical and Fujifilm. Author M.G. has contributed to advisory boards for Roche, Eisai, MSD and AZ. However, these activities have no potential conflicts of interest with the manuscript. None of the other authors have any potential conflicts (financial, professional or personal) that are relevant to the manuscript.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
