

Adverse Effects and Antibody Titers in Response to the BNT162b2 mRNA COVID-19 Vaccine in a Prospective Study of Healthcare Workers
- PMID: 35047649
- PMCID: PMC8759445
- DOI: 10.1093/ofid/ofab575
Adverse Effects and Antibody Titers in Response to the BNT162b2 mRNA COVID-19 Vaccine in a Prospective Study of Healthcare Workers
Abstract
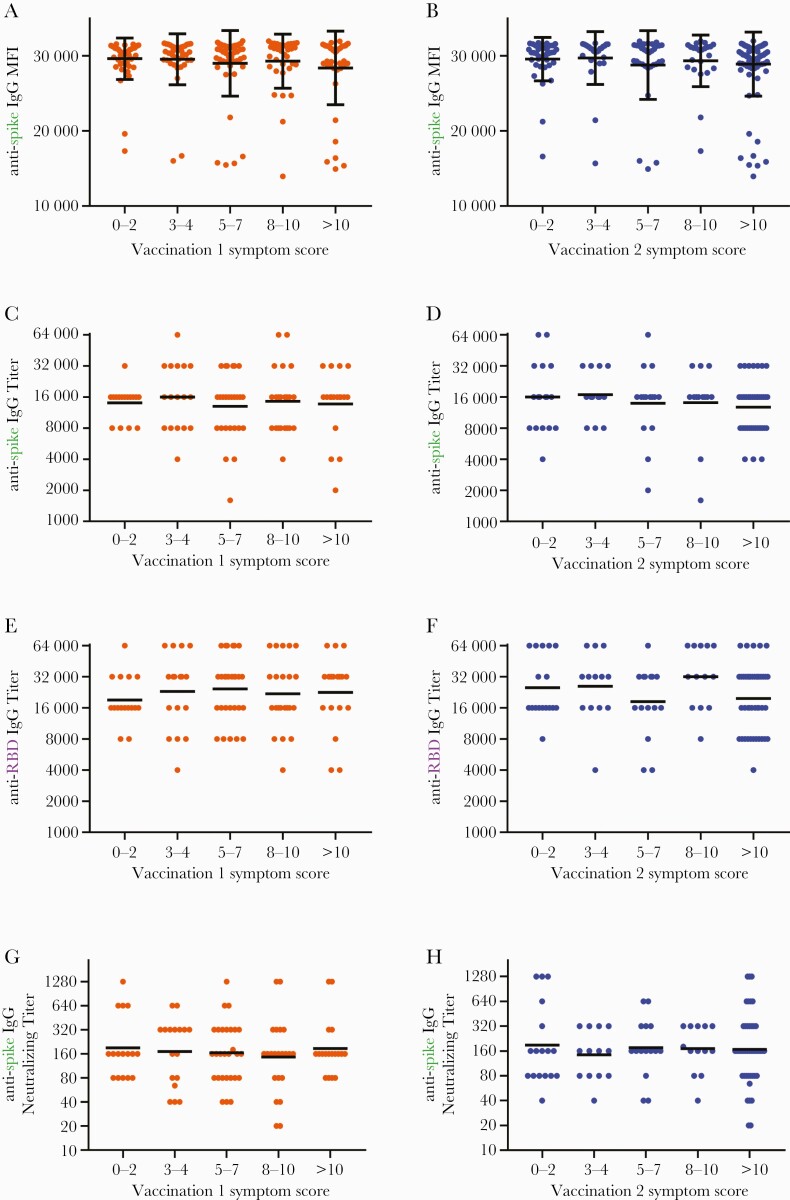
Background: The relationship between postvaccination symptoms and strength of antibody responses is unclear. The goal of this study was to determine whether adverse effects caused by vaccination with the Pfizer/BioNTech BNT162b2 vaccine are associated with the magnitude of vaccine-induced antibody levels.
Methods: We conducted a single-center, observational cohort study consisting of generally healthy adult participants that were not severely immunocompromised, had no history of coronavirus disease 2019, and were seronegative for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spike protein before vaccination. Severity of vaccine-associated symptoms was obtained through participant-completed questionnaires. Testing for immunoglobulin G antibodies against SARS-CoV-2 spike protein and receptor-binding domain was conducted using microsphere-based multiplex immunoassays performed on serum samples collected at monthly visits. Neutralizing antibody titers were determined by microneutralization assays.
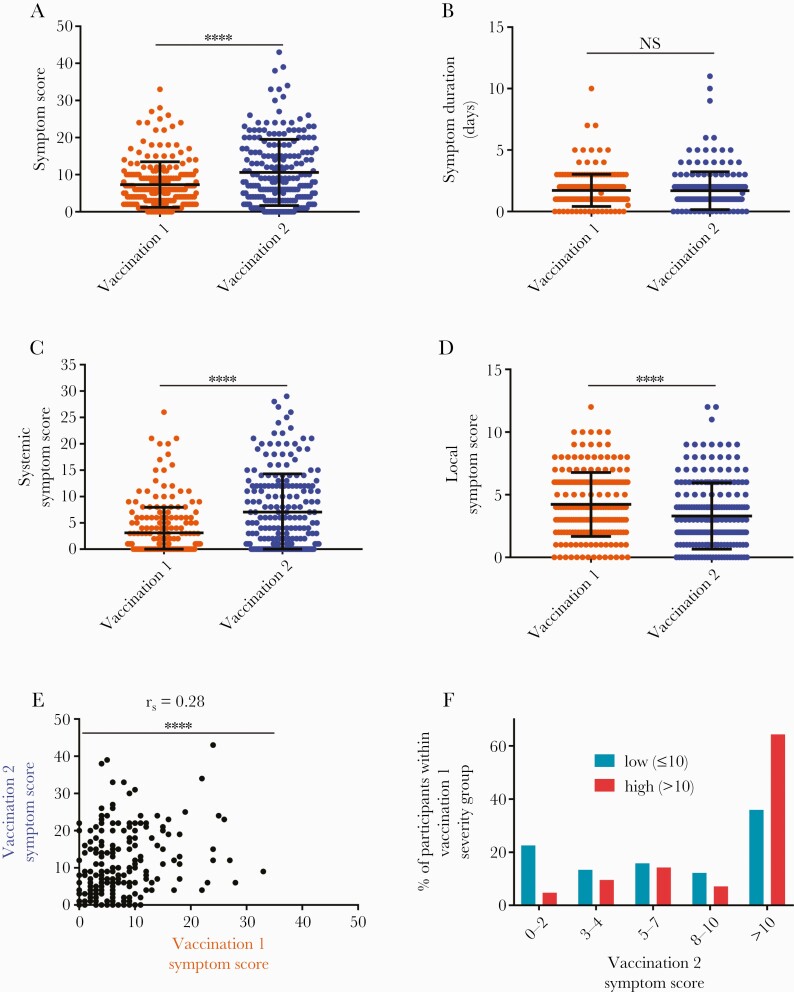
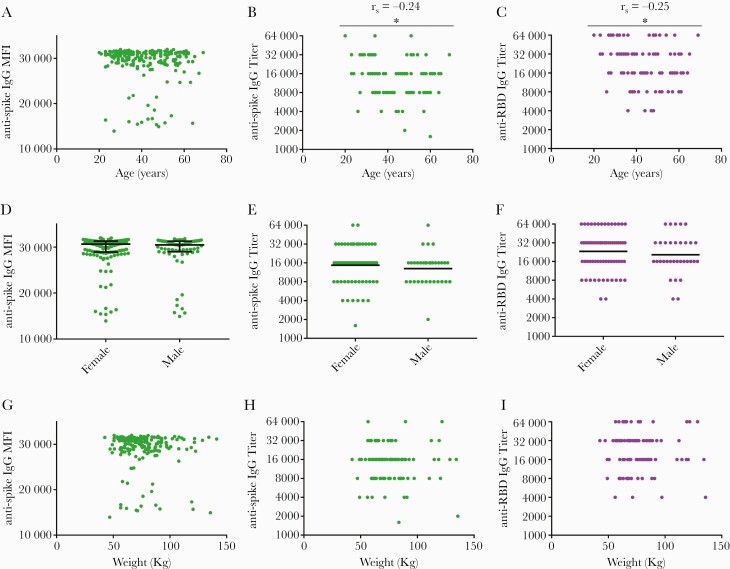
Results: Two hundred six participants were evaluated (69.4% female, median age 41.5 years old). We found no correlation between vaccine-associated symptom severity scores and vaccine-induced antibody titers 1 month after vaccination. We also observed that (1) postvaccination symptoms were inversely correlated with age and weight and more common in women, (2) systemic symptoms were more frequent after the second vaccination, (3) high symptom scores after first vaccination were predictive of high symptom scores after second vaccination, and (4) older age was associated with lower titers.
Conclusions: Lack of postvaccination symptoms after receipt of the BNT162b2 vaccine does not equate to lack of vaccine-induced antibodies 1 month after vaccination.
Keywords: COVID-19; SARS-CoV-2; adverse effects; antibody titer; mRNA vaccine.
Published by Oxford University Press on behalf of Infectious Diseases Society of America 2021.
Figures

Update of
-
Adverse effects and antibody titers in response to the BNT162b2 mRNA COVID-19 vaccine in a prospective study of healthcare workers.medRxiv [Preprint]. 2021 Jul 2:2021.06.25.21259544. doi: 10.1101/2021.06.25.21259544. medRxiv. 2021. Update in: Open Forum Infect Dis. 2021 Nov 20;9(1):ofab575. doi: 10.1093/ofid/ofab575. PMID: 34230937 Free PMC article. Updated. Preprint.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
