

Cardiac Catheterization and Hemodynamics in a Multicenter Cohort of Children with Pulmonary Hypertension
- PMID: 35049414
- PMCID: PMC9169121
- DOI: 10.1513/AnnalsATS.202108-998OC
Cardiac Catheterization and Hemodynamics in a Multicenter Cohort of Children with Pulmonary Hypertension
Abstract
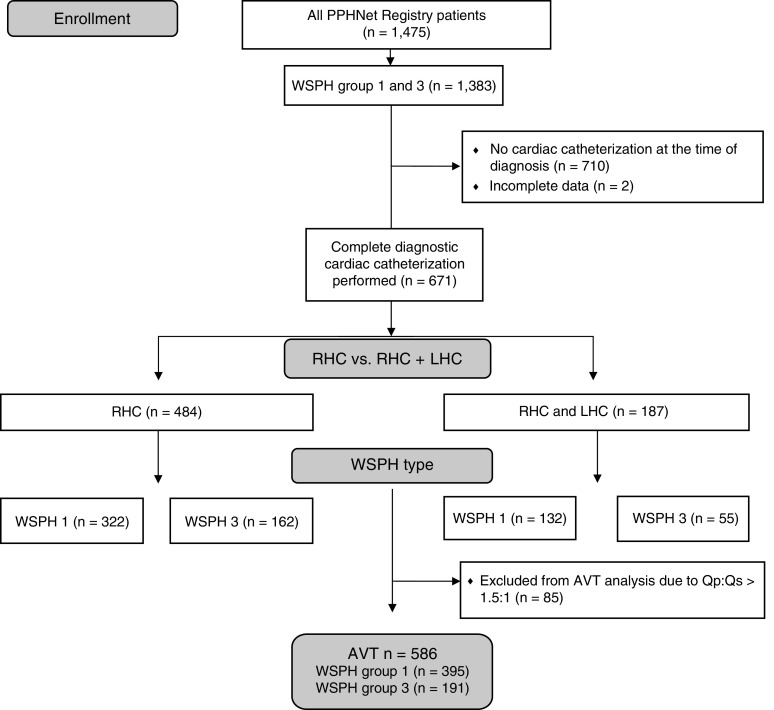
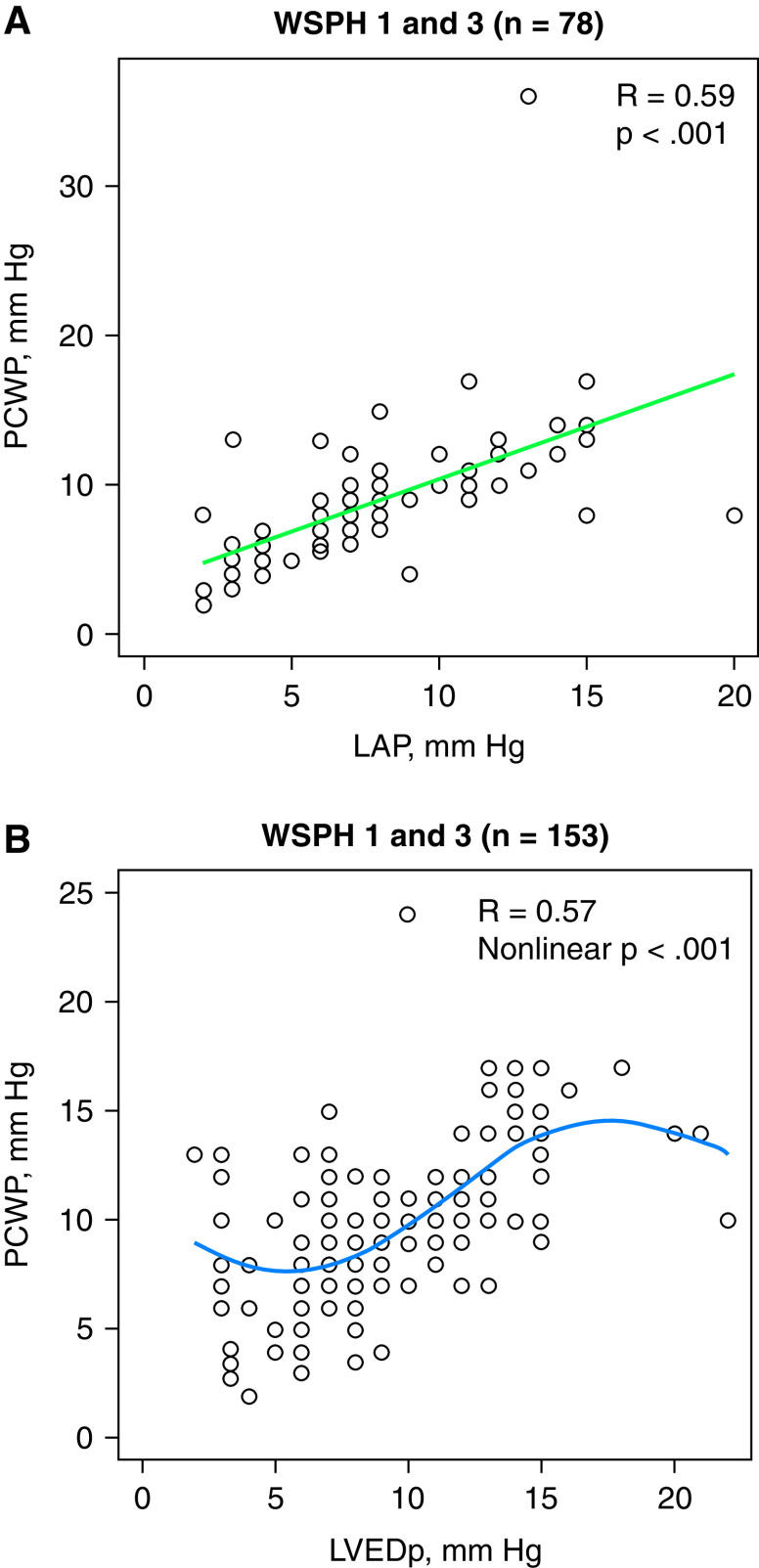
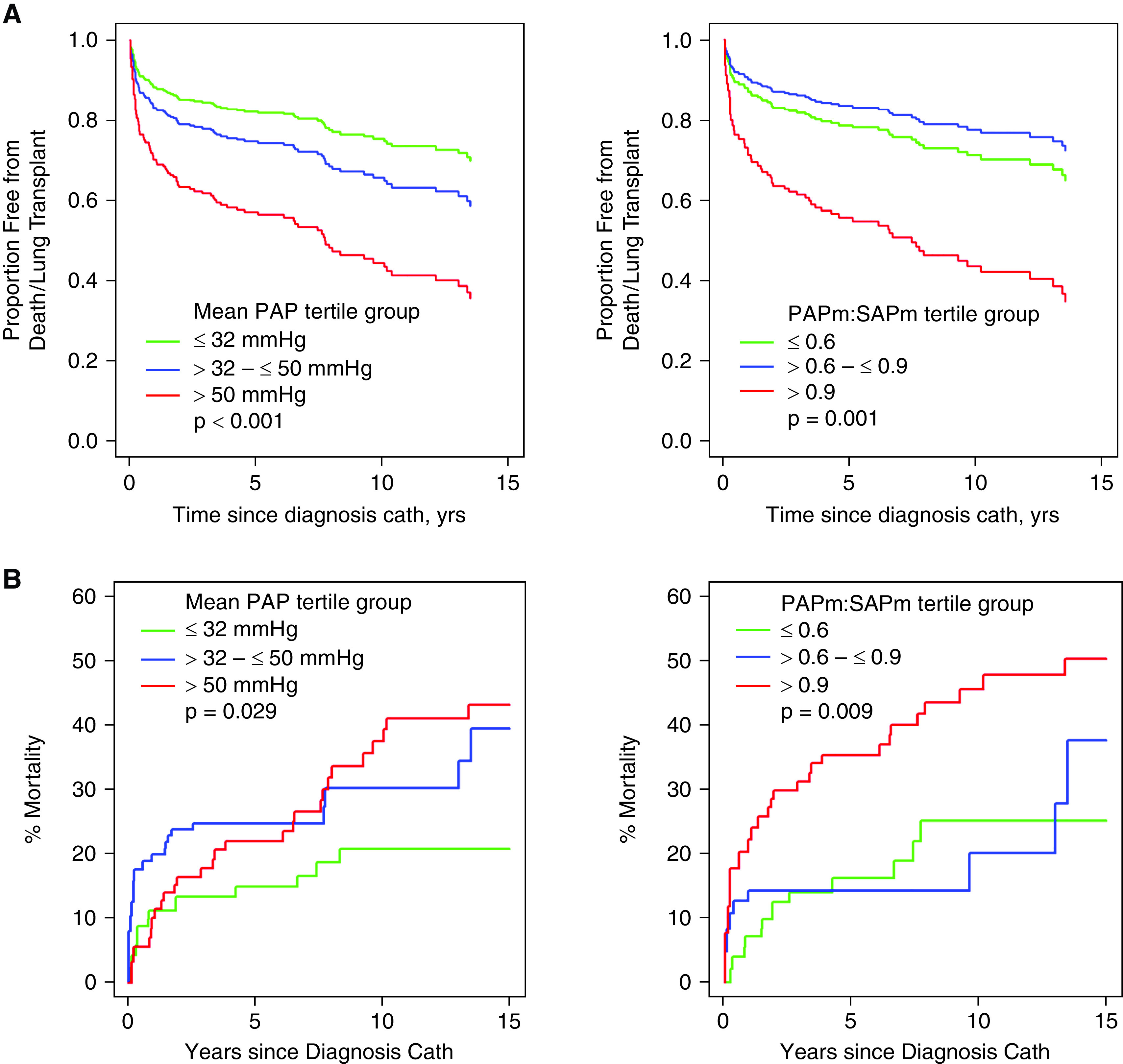
Rationale: Hemodynamic assessments direct care among children with pulmonary hypertension, yet the use of cardiac catheterization is highly variable, which could impact patient care and research. Objectives: We analyzed hemodynamic findings from right heart catheterization (RHC) and left heart catheterization and acute vasodilator testing (AVT) and the safety of catheterization in children with World Symposium on Pulmonary Hypertension (WSPH) group 1 and 3 subtypes in a large multicenter North American cohort. Methods: Of 1,475 children enrolled in the Pediatric Pulmonary Hypertension Network Registry (2014-2020), there were 1,383 group 1 and 3 patients, of whom 671 (48.5%) underwent RHC at diagnosis and were included for analysis. Results: Compared with those without diagnostic RHC, these children were older, less likely to be an infant or preterm, more often female, treated with targeted pulmonary hypertension medications at diagnosis, and had advanced World Health Organization functional class. Catheterization was performed without a difference in complication rates between WSPH groups. Pulmonary capillary wedge pressure was well correlated with left ventricular end-diastolic pressure and left atrial pressures. Results of AVT using three different methods were comparable; positive AVT results were observed in 8.0-11.8% of subjects, did not differ between WSPH groups 1 and 3, and were not associated with freedom from the composite endpoint of lung transplantation or death during follow-up. Conclusions: In a large pediatric pulmonary hypertension cohort, diagnostic RHC with or without left heart catheterization in WSPH group 1 and 3 patients was performed safely at experienced pediatric pulmonary hypertension centers. Hemodynamic differences were noted between group 1 and 3 subjects. Higher mean pulmonary arterial pressure and mean pulmonary arterial pressure/mean systemic arterial pressure ratio were associated with a higher risk of death/transplantation. Findings suggest overall safety and potential value of RHC as a standard diagnostic approach to guide pulmonary hypertension management in children.
Keywords: cardiac catheterization; hemodynamics; pediatrics; pulmonary hypertension; vasoreactivity testing.
Figures
References
-
- Matsuura H. Cardiac catheterization in children with pulmonary arterial hypertension. Pediatr Int (Roma) . 2017;59:3–9. - PubMed
-
- Bobhate P, Guo L, Jain S, Haugen R, Coe JY, Cave D, et al. Cardiac catheterization in children with pulmonary hypertensive vascular disease. Pediatr Cardiol . 2015;36:873–879. - PubMed
-
- Del Cerro MJ, Moledina S, Haworth SG, Ivy D, Al Dabbagh M, Banjar H, et al. Cardiac catheterization in children with pulmonary hypertensive vascular disease: consensus statement from the Pulmonary Vascular Research Institute, Pediatric and Congenital Heart Disease Task Forces. Pulm Circ . 2016;6:118–125. - PMC - PubMed
-
- Frank BS, Schäfer M, Grenolds A, Ivy DD, Abman SH, Darst JR. Acute vasoreactivity testing during cardiac catheterization of neonates with bronchopulmonary dysplasia-associated pulmonary hypertension. J Pediatr . 2019;208:127–133. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
