

The Neurokinin-1 Receptor Is a Target in Pediatric Rhabdoid Tumors
- PMID: 35049682
- PMCID: PMC8775224
- DOI: 10.3390/curroncol29010008
The Neurokinin-1 Receptor Is a Target in Pediatric Rhabdoid Tumors
Abstract
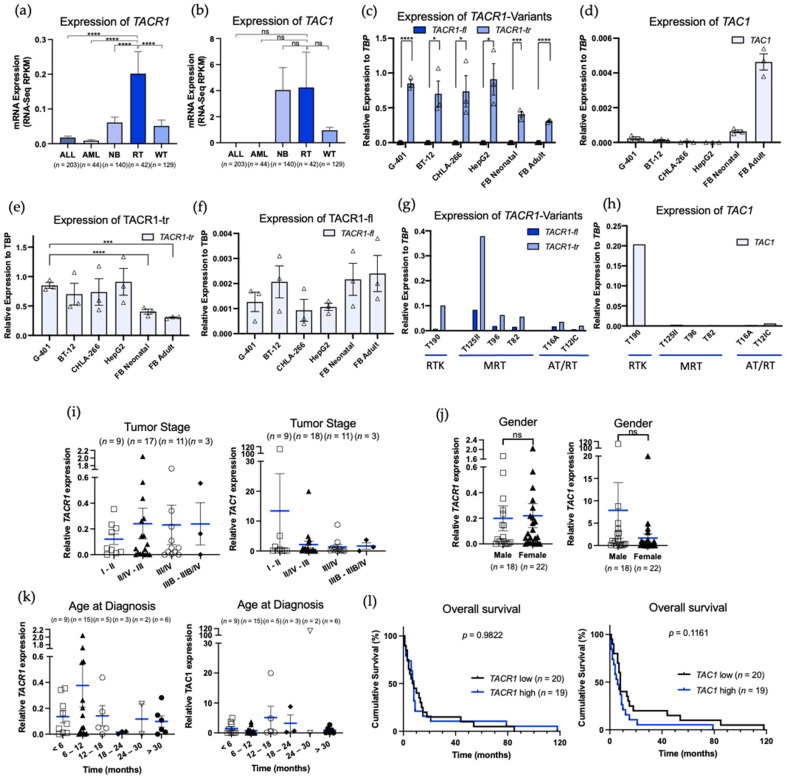
Rhabdoid tumors (RT) are among the most aggressive tumors in early childhood. Overall survival remains poor, and treatment only effectively occurs at the cost of high toxicity and late adverse effects. It has been reported that the neurokinin-1 receptor/ substance P complex plays an important role in cancer and proved to be a promising target. However, its role in RT has not yet been described. This study aims to determine whether the neurokinin-1 receptor is expressed in RT and whether neurokinin-1 receptor (NK1R) antagonists can serve as a novel therapeutic approach in treating RTs. By in silico analysis using the cBio Cancer Genomics Portal we found that RTs highly express neurokinin-1 receptor. We confirmed these results by RT-PCR in both tumor cell lines and in human tissue samples of various affected organs. We demonstrated a growth inhibitory and apoptotic effect of aprepitant in viability assays and flow cytometry. Furthermore, this effect proved to remain when used in combination with the cytostatic cisplatin. Western blot analysis showed an upregulation of apoptotic signaling pathways in rhabdoid tumors when treated with aprepitant. Overall, our findings suggest that NK1R may be a promising target for the treatment of RT in combination with other anti-cancer therapies and can be targeted with the NK1R antagonist aprepitant.
Keywords: NK-1 receptor; NK-1 receptor antagonist; apoptosis; cancer; rhabdoid tumor; substance P.
Conflict of interest statement
S.K. has received honoraria from Novartis, TCR2 and GSK. S.K. is an inventor of several patents in the field of immuno-oncology. S.K. received research support from TCR2 Inc and Arcus Bioscience for work unrelated to this manuscript.
Figures



References
-
- Chi S.N., Zimmerman M.A., Yao X., Cohen K.J., Burger P., Biegel J.A., Rorke-Adams L.B., Fisher M.J., Janss A., Mazewski C., et al. Intensive multimodality treatment for children with newly diagnosed CNS atypical teratoid rhabdoid tumor. J. Clin. Oncol. 2009;27:385–389. doi: 10.1200/JCO.2008.18.7724. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
