

Impact of Pre-Treatment NLR and Other Hematologic Biomarkers on the Outcomes of Early-Stage Non-Small-Cell Lung Cancer Treated with Stereotactic Body Radiation Therapy
- PMID: 35049693
- PMCID: PMC8774597
- DOI: 10.3390/curroncol29010019
Impact of Pre-Treatment NLR and Other Hematologic Biomarkers on the Outcomes of Early-Stage Non-Small-Cell Lung Cancer Treated with Stereotactic Body Radiation Therapy
Abstract
Introduction: We evaluated the association of pre-treatment immunologic biomarkers on the outcomes of early-stage non-small-cell lung cancer (NSCLC) patients treated with stereotactic body radiation therapy (SBRT).
Materials and methods: In this retrospective study, all newly diagnosed early-stage NSCLC treated with SBRT between January 2010 and December 2017 were screened and included for further analysis. The pre-treatment neutrophil-lymphocyte ratio (NLR), monocyte lymphocyte ratio (MLR), and platelet-lymphocyte ratio (PLR) were calculated. Overall survival (OS) and recurrence-free survival (RFS) were estimated by Kaplan-Meier. Multivariable models were constructed to determine the impact of different biomarkers and the Akaike information criterion (AIC), index of adequacy, and scaled Brier scores were calculated.
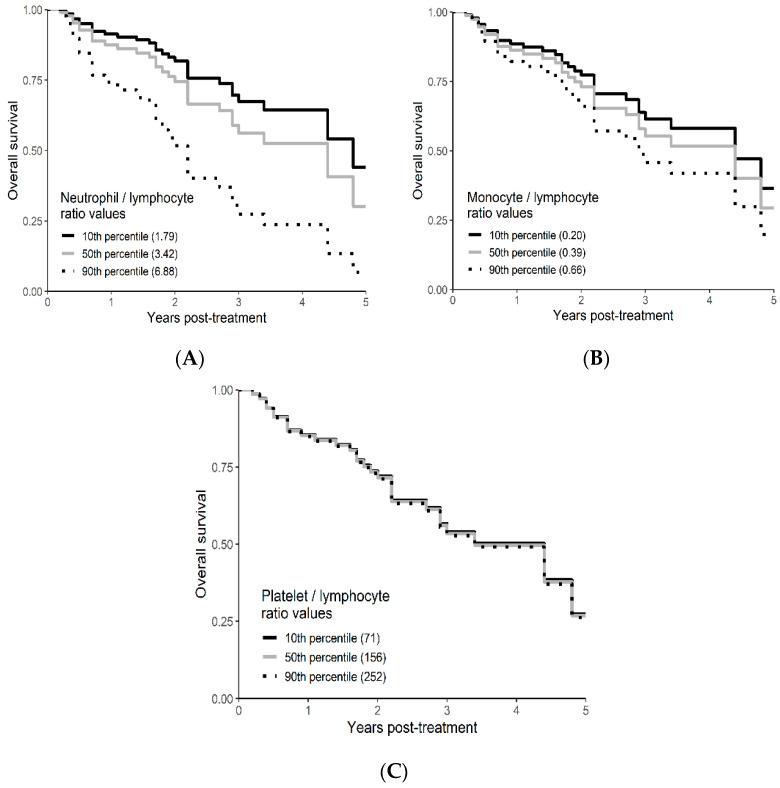
Results: A total of 72 patients were identified and 61 were included in final analysis. The median neutrophil count at baseline was 5.4 × 109/L (IQR: 4.17-7.05 × 109/L). Median lymphocyte count was 1.63 × 109/L (IQR: 1.29-2.10 × 109/L), median monocyte count was 0.65 × 109/L (IQR: 0.54-0.83 × 109/L), median platelet count was 260.0 × 109/L (IQR: 211.0-302.0 × 109/L). The median NLR was 3.42 (IQR: 2.38-5.04), median MLR was 0.39 (IQR: 0.31-0.53), and median PLR was 156.4 (IQR: 117.2-197.5). On multivariable regression a higher NLR was associated with worse OS (p = 0.01; HR-1.26; 95% CI 1.04-1.53). The delta AIC between the two multivariable models was 3.4, suggesting a moderate impact of NLR on OS. On multivariable analysis, higher NLR was associated with poor RFS (p = 0.001; NLR^1 HR 0.36; 0.17-0.78; NLR^2 HR-1.16; 95% CI 1.06-1.26) with a nonlinear relationship. The delta AIC between the two multivariable models was 16.2, suggesting a strong impact of NLR on RFS. In our cohort, MLR and PLR were not associated with RFS or OS in multivariable models.
Conclusions: Our study suggests NLR, as a biomarker of systemic inflammation, is an independent prognostic factor for OS and RFS. The nonlinear relationship with RFS may indicate a suitable immunological environment is needed for optimal SBRT action and tumoricidal mechanisms. These findings require further validation in independent cohorts.
Keywords: biomarkers; early-stage lung cancer; stereotactic body radiation therapy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures









References
-
- Chang J.Y., Senan S., Paul M.A., Mehran R.J., Louie A.V., Balter P., Groen H.J.M., E McRae S.E., Widder J., Feng L., et al. Stereotactic ablative radiotherapy versus lobectomy for operable stage I non-small-cell lung cancer: A pooled analysis of two randomised trials. Lancet Oncol. 2015;16:630–637. doi: 10.1016/S1470-2045(15)70168-3. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
