

Renin Angiotensin System Blockers and Risk of Mortality in Hypertensive Patients Hospitalized for COVID-19: An Italian Registry
- PMID: 35050225
- PMCID: PMC8781822
- DOI: 10.3390/jcdd9010015
Renin Angiotensin System Blockers and Risk of Mortality in Hypertensive Patients Hospitalized for COVID-19: An Italian Registry
Abstract
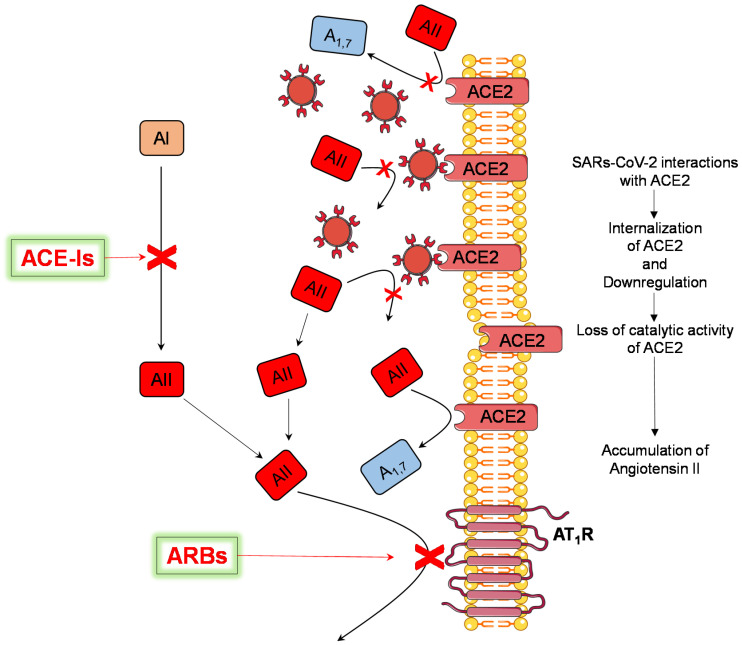
Background: It is uncertain whether exposure to renin-angiotensin system (RAS) modifiers affects the severity of the new coronavirus disease 2019 (COVID-19) because most of the available studies are retrospective.
Methods: We tested the prognostic value of exposure to RAS modifiers (either angiotensin-converting enzyme inhibitors [ACE-Is] or angiotensin receptor blockers [ARBs]) in a prospective study of hypertensive patients with COVID-19. We analyzed data from 566 patients (mean age 75 years, 54% males, 162 ACE-Is users, and 147 ARBs users) hospitalized in five Italian hospitals. The study used systematic prospective data collection according to a pre-specified protocol. All-cause mortality during hospitalization was the primary outcome.
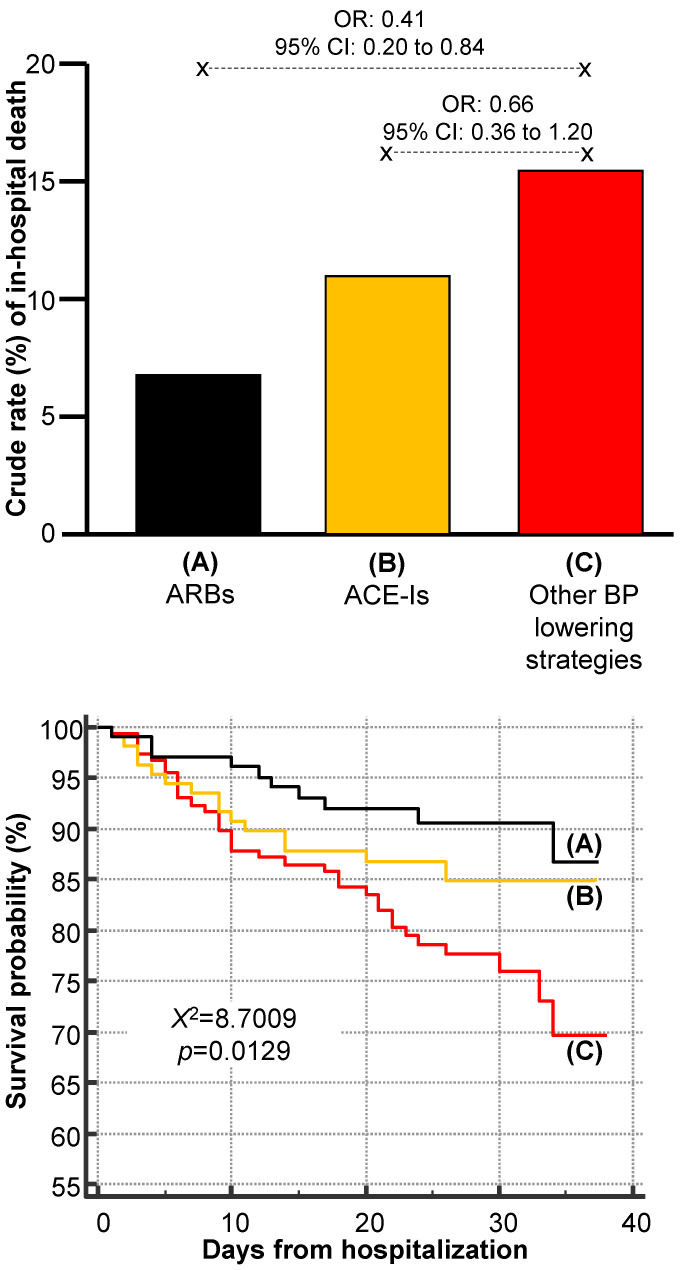
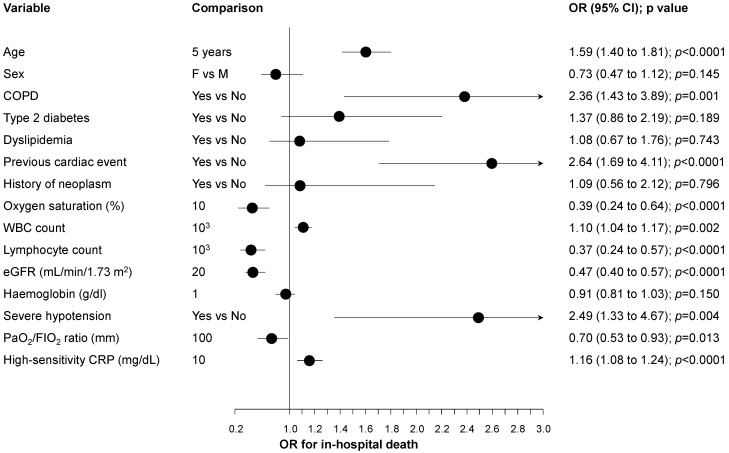
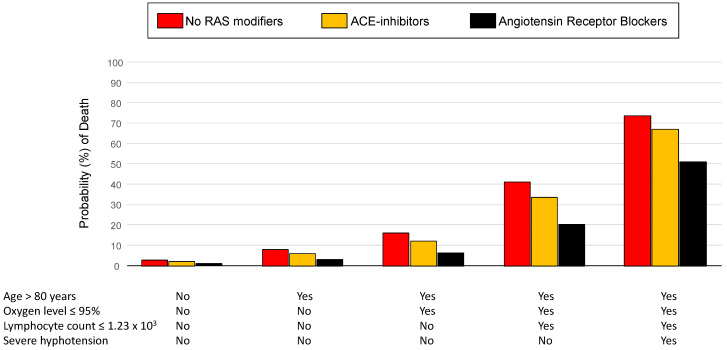
Results: Sixty-six patients died during hospitalization. Exposure to RAS modifiers was associated with a significant reduction in the risk of in-hospital mortality when compared to other BP-lowering strategies (odds ratio [OR]: 0.54, 95% confidence interval [CI]: 0.32 to 0.90, p = 0.019). Exposure to ACE-Is was not significantly associated with a reduced risk of in-hospital mortality when compared with patients not treated with RAS modifiers (OR: 0.66, 95% CI: 0.36 to 1.20, p = 0.172). Conversely, ARBs users showed a 59% lower risk of death (OR: 0.41, 95% CI: 0.20 to 0.84, p = 0.016) even after allowance for several prognostic markers, including age, oxygen saturation, occurrence of severe hypotension during hospitalization, and lymphocyte count (adjusted OR: 0.37, 95% CI: 0.17 to 0.80, p = 0.012). The discontinuation of RAS modifiers during hospitalization did not exert a significant effect (p = 0.515).
Conclusions: This prospective study indicates that exposure to ARBs reduces mortality in hospitalized patients with COVID-19.
Keywords: ACE inhibitors; ACE2; COVID-19; SARS-CoV-2; angiotensin receptor blockers; angiotensin-converting enzyme inhibitors; renin–angiotensin system.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous
