

Causes and timing of 30-day rehospitalization from skilled nursing facilities after a hospital admission for pneumonia or sepsis
- PMID: 35051181
- PMCID: PMC8775208
- DOI: 10.1371/journal.pone.0260664
Causes and timing of 30-day rehospitalization from skilled nursing facilities after a hospital admission for pneumonia or sepsis
Abstract
Background: Pneumonia and sepsis are among the most common causes of hospitalization in the United States and often result in discharges to a skilled nursing facility (SNF) for rehabilitation. We described the timing and most common causes of 30-day unplanned hospital readmission following an index hospitalization for pneumonia or sepsis.
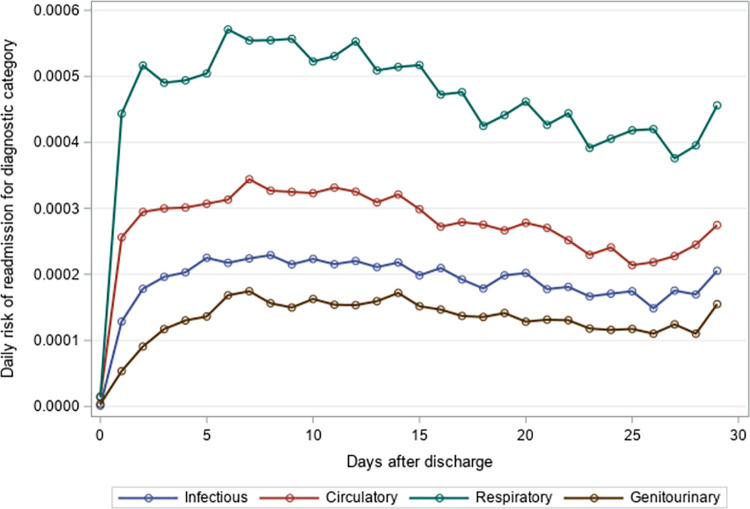
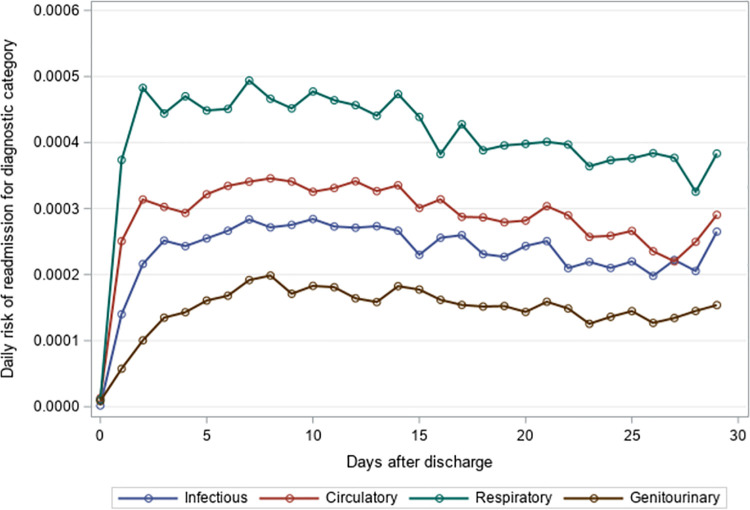
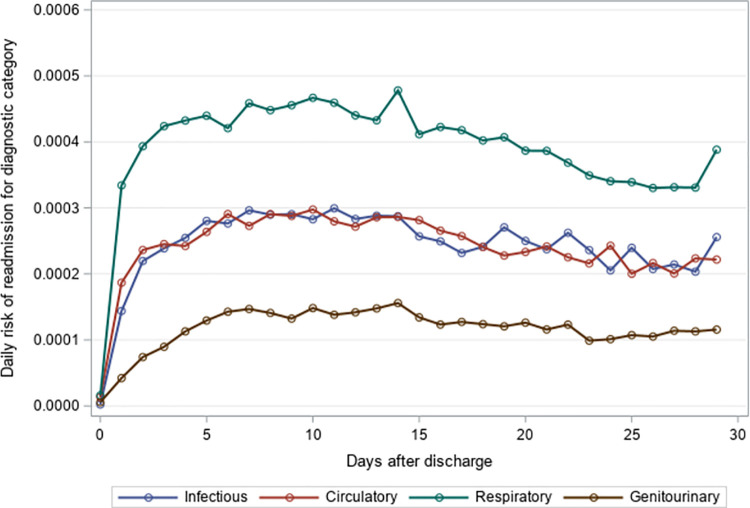
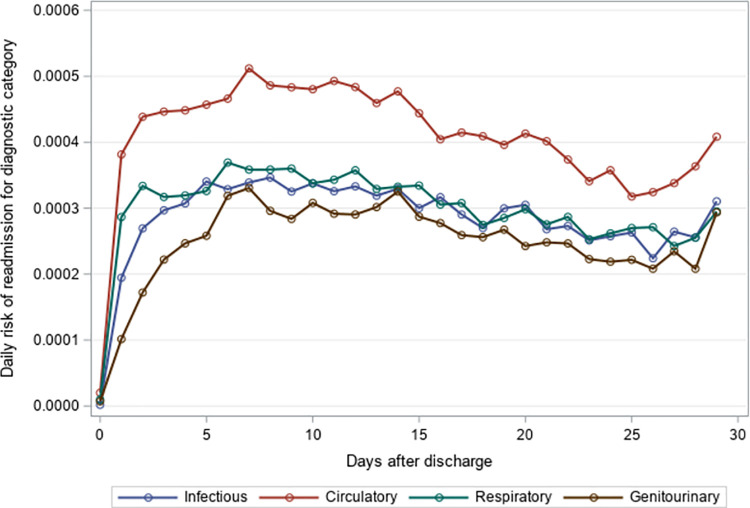
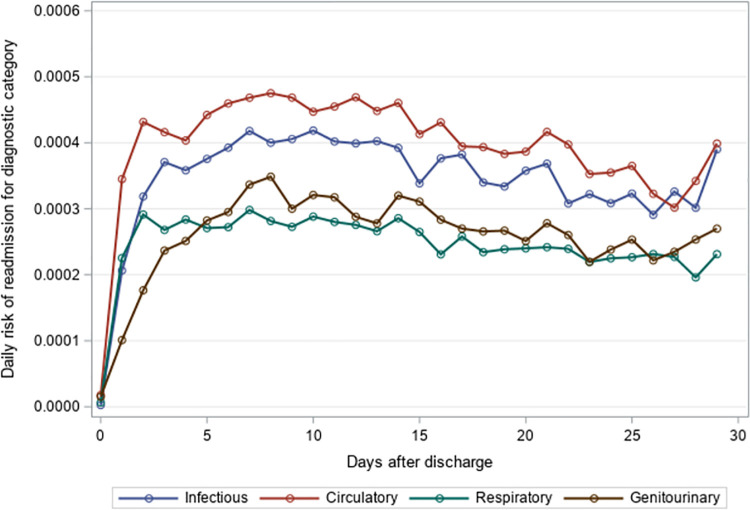
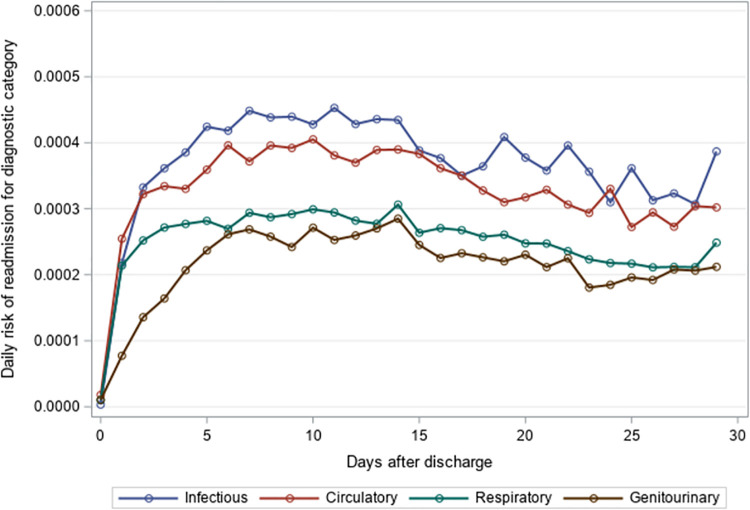
Methods and findings: This national retrospective cohort study included adults ≥65 years who were hospitalized for pneumonia or sepsis and were discharged to a SNF between July 1, 2012 and July 4, 2015. We quantified the ten most common 30-day unplanned readmission diagnoses and estimated the daily risk of first unplanned rehospitalization for four causes of readmission (circulatory, infectious, respiratory, and genitourinary). The index hospitalization was pneumonia for 92,153 SNF stays and sepsis for 452,254 SNF stays. Of these SNF stays, 20.9% and 25.9%, respectively, resulted in a 30-day unplanned readmission. Overall, septicemia was the single most common readmission diagnosis for residents with an index hospitalization for pneumonia (16.7% of 30-day readmissions) and sepsis (22.4% of 30-day readmissions). The mean time to unplanned readmission was approximately 14 days overall. Respiratory causes displayed the highest daily risk of rehospitalization following index hospitalizations for pneumonia, while circulatory and infectious causes had the highest daily risk of rehospitalization following index hospitalizations for sepsis. The day of highest risk for readmission occurred within two weeks of the index hospitalization discharge, but the readmission risk persisted across the 30-day follow-up.
Conclusion: Among older adults discharged to SNFs following a hospitalization for pneumonia or sepsis, hospital readmissions for infectious, circulatory, respiratory, and genitourinary causes occurred frequently throughout the 30-day post-discharge period. Our data suggests further study is needed, perhaps on the value of closer monitoring in SNFs post-hospital discharge and improved communication between hospitals and SNFs, to reduce the risk of potentially preventable hospital readmissions.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: R.V.A. and A.C. are employed by Sanofi Pasteur and may hold shares and/or stock options in the company. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
Similar articles
-
Variation in Postsepsis Readmission Patterns: A Cohort Study of Veterans Affairs Beneficiaries.Ann Am Thorac Soc. 2017 Feb;14(2):230-237. doi: 10.1513/AnnalsATS.201605-398OC. Ann Am Thorac Soc. 2017. PMID: 27854510 Free PMC article.
-
Home Health Care After Skilled Nursing Facility Discharge Following Heart Failure Hospitalization.J Am Geriatr Soc. 2020 Jan;68(1):96-102. doi: 10.1111/jgs.16179. Epub 2019 Oct 11. J Am Geriatr Soc. 2020. PMID: 31603248 Free PMC article.
-
Risk of Readmission After Discharge From Skilled Nursing Facilities Following Heart Failure Hospitalization: A Retrospective Cohort Study.J Am Med Dir Assoc. 2019 Apr;20(4):432-437. doi: 10.1016/j.jamda.2019.01.135. J Am Med Dir Assoc. 2019. PMID: 30954133 Free PMC article.
-
Reducing Hospital Readmissions of Older Adults Pursuing Postacute Care at Skilled Nursing Facilities: A Scoping Review.Am J Occup Ther. 2022 Jan 1;76(1):7601180130. doi: 10.5014/ajot.2022.049082. Am J Occup Ther. 2022. PMID: 34997839
-
Hospital readmission of skilled nursing facility residents: a systematic review.Res Gerontol Nurs. 2015 May-Jun;8(3):148-56. doi: 10.3928/19404921-20150129-01. Epub 2015 Feb 24. Res Gerontol Nurs. 2015. PMID: 25710452
Cited by
-
Impact of skilled nursing facility discharge on inpatient oncology quality outcomes.JNCI Cancer Spectr. 2025 Apr 30;9(3):pkaf055. doi: 10.1093/jncics/pkaf055. JNCI Cancer Spectr. 2025. PMID: 40408163 Free PMC article.
References
-
- Torio C (AHRQ), Moore B (Truven Health Analytics). National Inpatient Hospital Costs: The Most Expensive Conditions by Payer, 2013. HCUP Statistical Brief #204. May 2016. Agency for Healthcare Research and Quality, Rockville, MD. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb204-Most-Expensive-Hosp.... - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
