

Leading causes of death and high mortality rates in an HIV endemic setting (Kisumu county, Kenya, 2019)
- PMID: 35051186
- PMCID: PMC8775329
- DOI: 10.1371/journal.pone.0261162
Leading causes of death and high mortality rates in an HIV endemic setting (Kisumu county, Kenya, 2019)
Abstract
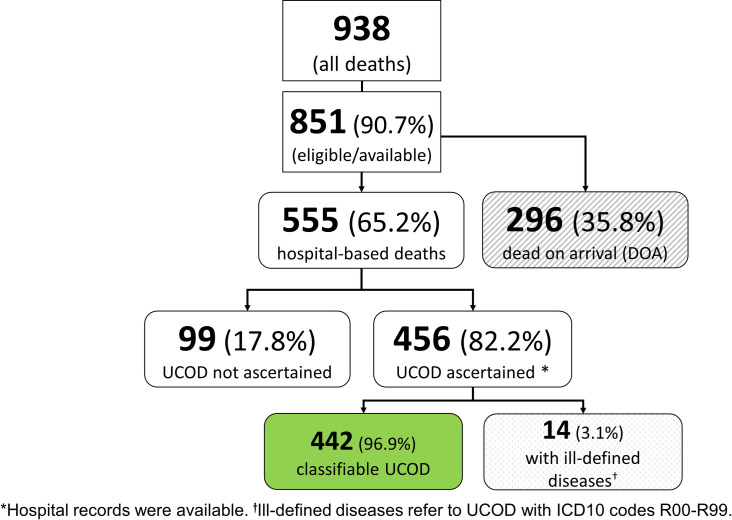
Background: In resource-limited settings, underlying causes of death (UCOD) often are not ascertained systematically, leading to unreliable mortality statistics. We reviewed medical charts to establish UCOD for decedents at two high volume mortuaries in Kisumu County, Kenya, and compared ascertained UCOD to those notified to the civil registry.
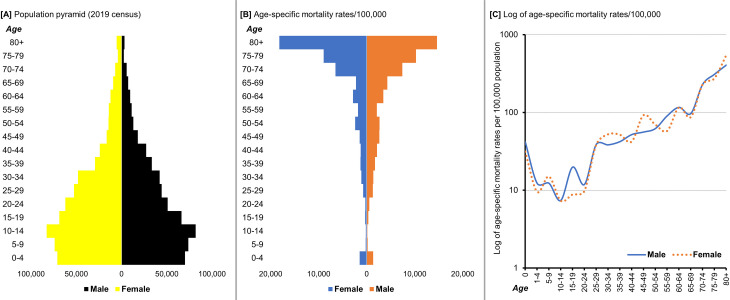
Methods: Medical experts trained in COD certification examined medical charts and ascertained causes of death for 456 decedents admitted to the mortuaries from April 16 through July 12, 2019. Decedents with unknown HIV status or who had tested HIV-negative >90 days before the date of death were tested for HIV. We calculated annualized all-cause and cause-specific mortality rates grouped according to global burden of disease (GBD) categories and separately for deaths due to HIV/AIDS and expressed estimated deaths per 100,000 population. We compared notified to ascertained UCOD using Cohen's Kappa (κ) and assessed for the independence of proportions using Pearson's chi-squared test.
Findings: The four leading UCOD were HIV/AIDS (102/442 [23.1%]), hypertensive disease (41/442 [9.3%]), other cardiovascular diseases (23/442 [5.2%]), and cancer (20/442 [4.5%]). The all-cause mortality rate was 1,086/100,000 population. The highest cause-specific mortality was in GBD category II (noncommunicable diseases; 516/100,000), followed by GBD I (communicable, perinatal, maternal, and nutritional; 513/100,000), and III (injuries; 56/100,000). The HIV/AIDS mortality rate was 251/100,000 population. The proportion of deaths due to GBD II causes was higher among females (51.9%) than male decedents (42.1%; p = 0.039). Conversely, more men/boys (8.6%) than women/girls (2.1%) died of GBD III causes (p = 0.002). Most of the records with available recorded and ascertained UCOD (n = 236), 167 (70.8%) had incorrectly recorded UCOD, and agreement between notified and ascertained UCOD was poor (29.2%; κ = 0.26).
Conclusions: Mortality from infectious diseases, especially HIV/AIDS, is high in Kisumu County, but there is a shift toward higher mortality from noncommunicable diseases, possibly reflecting an epidemiologic transition and improving HIV outcomes. The epidemiologic transition suggests the need for increased focus on controlling noncommunicable conditions despite the high communicable disease burden. The weak agreement between notified and ascertained UCOD could lead to substantial inaccuracies in mortality statistics, which wholly depend on death notifications.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
High HIV prevalence among decedents received by two high-volume mortuaries in Kisumu, western Kenya, 2019.PLoS One. 2021 Jul 1;16(7):e0253516. doi: 10.1371/journal.pone.0253516. eCollection 2021. PLoS One. 2021. PMID: 34197509 Free PMC article.
-
All-cause and cause-specific mortality rates for Kisumu County: a comparison with Kenya, low-and middle-income countries.BMC Public Health. 2022 Sep 27;22(1):1828. doi: 10.1186/s12889-022-14141-5. BMC Public Health. 2022. PMID: 36167543 Free PMC article.
-
A review of completeness, correctness, and order of cause of death statements among decedents with documented causes of death and HIV status at two major mortuaries in Kenya, 2015.J Forensic Leg Med. 2020 Jul;73:101993. doi: 10.1016/j.jflm.2020.101993. Epub 2020 Jun 2. J Forensic Leg Med. 2020. PMID: 32658751 Free PMC article.
-
Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019.Lancet Psychiatry. 2022 Feb;9(2):137-150. doi: 10.1016/S2215-0366(21)00395-3. Epub 2022 Jan 10. Lancet Psychiatry. 2022. PMID: 35026139 Free PMC article.
-
Global and regional causes of death.Br Med Bull. 2009;92:7-32. doi: 10.1093/bmb/ldp028. Br Med Bull. 2009. PMID: 19776034 Review.
Cited by
-
Estimated contributions and future mitigation strategies for HIV risk around funeral practices in western Kenya: a mathematical modeling study.BMC Med. 2025 Feb 12;23(1):85. doi: 10.1186/s12916-025-03907-4. BMC Med. 2025. PMID: 39939974 Free PMC article.
-
Perceptions of body size and non-communicable disease risk among people with HIV in Nairobi, Kenya: an explanatory mixed-methods study.BMJ Glob Health. 2025 Jul 31;10(7):e016546. doi: 10.1136/bmjgh-2024-016546. BMJ Glob Health. 2025. PMID: 40744671 Free PMC article.
References
-
- World Health Organization. The Global Burden of Disease: Summary. 1996.
-
- Mathers CD, Stein C, Fat DM, Rao C, Inoue M, Tomijima N, et al.. Global burden of disease 2000: version 2 methods and results. 2002.
-
- United Nations Department of Economic and Social Affairs. World Population Prospects 2019. https://population.un.org/wpp/Download/Standard/Mortality/ (accessed May 21, 2020).
-
- Achoki T, Miller-Petrie MK, Glenn SD, Kalra N, Lesego A, Gathecha GK, et al.. Health disparities across the counties of Kenya and implications for policy makers, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Glob Heal 2019;7:e81–95. doi: 10.1016/S2214-109X(18)30472-8 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
