

The global prevalence and ethnic heterogeneity of primary ciliary dyskinesia gene variants: a genetic database analysis
- PMID: 35051411
- PMCID: PMC9064931
- DOI: 10.1016/S2213-2600(21)00453-7
The global prevalence and ethnic heterogeneity of primary ciliary dyskinesia gene variants: a genetic database analysis
Abstract
Background: Primary ciliary dyskinesia (PCD) is a motile ciliopathy characterised by otosinopulmonary infections. Inheritance is commonly autosomal recessive, with extensive locus and allelic heterogeneity. The prevalence is uncertain. Most genetic studies have been done in North America or Europe. The aim of the study was to estimate the worldwide prevalence and ethnic heterogeneity of PCD.
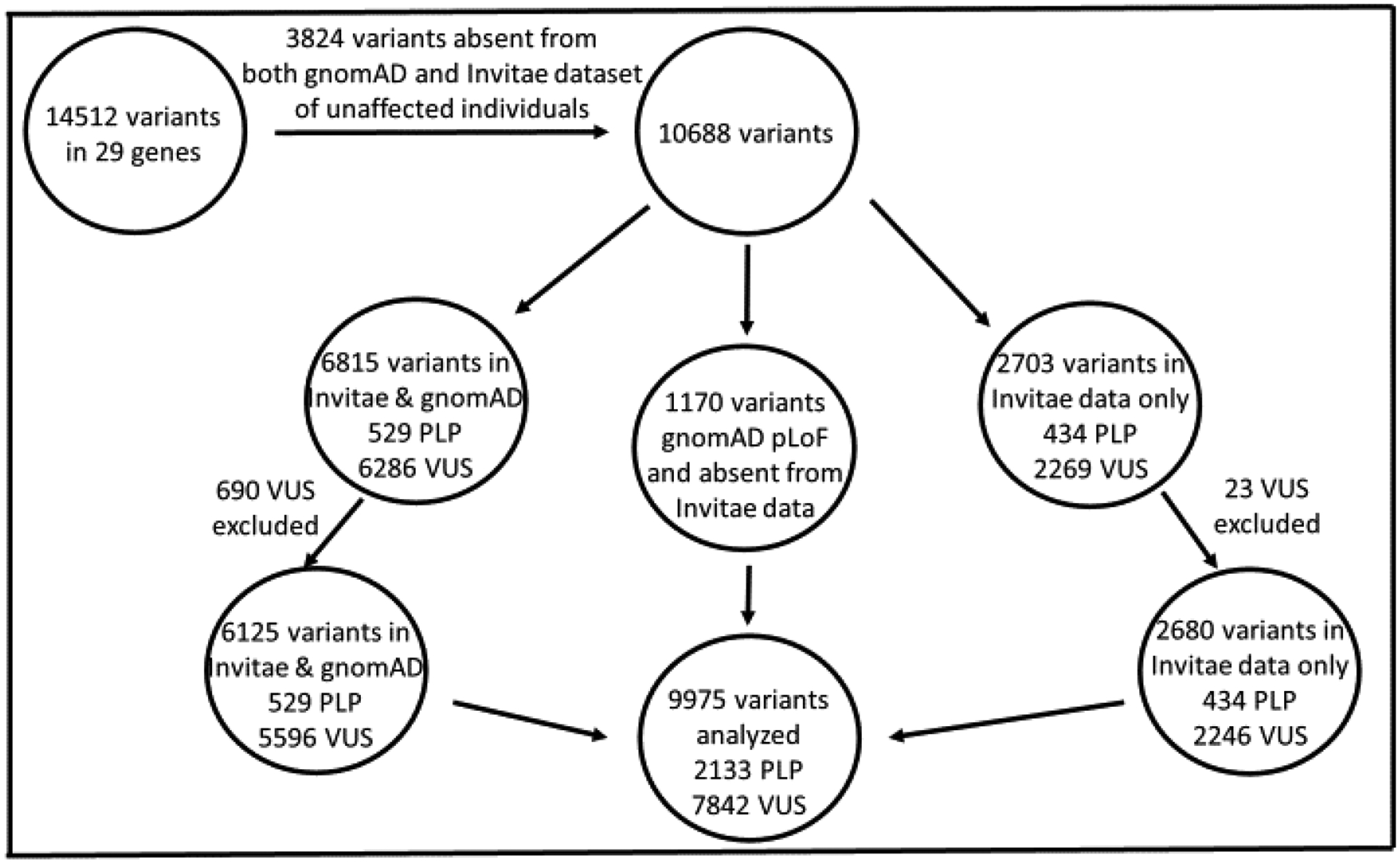
Methods: We calculated the allele frequency of disease-causing variants in 29 PCD genes associated with autosomal recessive inheritance in 182 681 unique individuals to estimate the global prevalence of PCD in seven ethnicities (African or African American, Latino, Ashkenazi Jewish, Finnish, non-Finnish European, east Asian, and south Asian). We began by aggregating variants that had been interpreted by Invitae, San Francisco, CA, USA, a genetics laboratory with PCD expertise. We then determined the allele frequency of each variant (pathogenic, likely pathogenic, or variant of uncertain significance [VUS]) in the Genome Aggregation Database (gnomAD), a publicly available next-generation sequencing database that aggregates exome and genome sequencing information from a wide variety of large-scale projects and stratifies allele counts by ethnicity. Using the Hardy-Weinberg equilibrium equation, we were able to calculate a lower-end prevalence of PCD for each ethnicity by including only pathogenic and likely pathogenic variants; and upper-end prevalence by also including VUS. This approach was similar to previous work on Li-Fraumeni (TP53 variants) prevalence. We were not diagnosing PCD, but rather estimating prevalence based on known variants.
Findings: The overall minimum global prevalence of PCD is calculated to be at least one in 7554 individuals, although this is likely to be an underestimate because some variants currently classified as VUS might be disease-causing and some pathogenic variants might not be detected by our methods. In the overall cohort, Invitae data could be included for variants without gnomAD data for a primary ethnicity. When using only gnomAD allele frequencies to calculate prevalence in individual ethnicities, the estimated prevalence of PCD was lower in each ethnicity compared with the overall cohort. This is because the overall cohort includes additional data from the Invitae database such as copy number variants and other variants not present in gnomAD. With gnomAD we found the expected PCD frequency to be higher in individuals of African ancestry than in most other populations (excluding VUS: 1 in 9906 in African or African American vs 1 in 10 388 in non-Finnish European vs 1 in 14 606 in east Asian vs 1 in 16 309 in Latino; including VUS: 1 in 106 in African or African American vs 1 in 178 in non-Finnish European vs 1 in 196 in Latino vs 1 in 188 in east Asian). In addition, we found that the top 5 genes most commonly implicated in PCD differed across ethnic ancestries and contrasted commonly published findings.
Interpretation: PCD appears to be more common than has been recognised, particularly in individuals of African ancestry. We identified gene distributions that differ from those in previous European and North American studies. These results could have an international impact on case identification. Our analytic approach can be expanded as more PCD loci are identified, and could be adapted to study the prevalence of other inherited diseases.
Funding: None.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests WBH receives support from the National Institutes of Health (NIH) Loan Repayment Program, outside of the submitted work. BAS reports other from Duke University School of Medicine (salary from ABMGG Laboratory Genetics and Genomics Fellowship), other from Medical Science and Computing (salary as Clinical Molecular Geneticist contractor at the National Institute of Allergy and Infectious Diseases [NIAID] and NIH), and other from American College of Medical Genetics and Genomics (ACMG; US$100 000, registration, travel, and transportation fees to attend ACMG Annual Meeting as the 2019 Richard King Trainee Awardee), outside of the submitted work. RT and KN are employees and stockholders at Invitae—a genetic testing provider offering testing for Primary Ciliary Dyskinesia. MAZ has salary support from research grants from NIH, outside of the submitted work. BG received salary support from research grants from NIH, outside of the submitted work. KA and YZ declare no competing interests.
Figures


Comment in
-
Primary ciliary dyskinesia: a big data genomics approach.Lancet Respir Med. 2022 May;10(5):423-425. doi: 10.1016/S2213-2600(22)00009-1. Epub 2022 Jan 17. Lancet Respir Med. 2022. PMID: 35051410 No abstract available.
References
-
- Zariwala MA, Knowles MR, Leigh MW. Primary Ciliary Dyskinesia. 2007. Jan 24 [Updated 2019 Dec 5]. In: Adam MP, Ardinger HH, Pagon RA, et al. , editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2019. Available from: https://www.ncbi.nlm.nih.gov/books/NBK1122/ - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
