

Movement Disorders in Oncology: From Clinical Features to Biomarkers
- PMID: 35052708
- PMCID: PMC8772745
- DOI: 10.3390/biomedicines10010026
Movement Disorders in Oncology: From Clinical Features to Biomarkers
Abstract
Background: the study of movement disorders associated with oncological diseases and anticancer treatments highlights the wide range of differential diagnoses that need to be considered. In this context, the role of immune-mediated conditions is increasingly recognized and relevant, as they represent treatable disorders.
Methods: we reappraise the phenomenology, pathophysiology, diagnostic testing, and treatment of movement disorders observed in the context of brain tumors, paraneoplastic conditions, and cancer immunotherapy, such as immune-checkpoint inhibitors (ICIs).
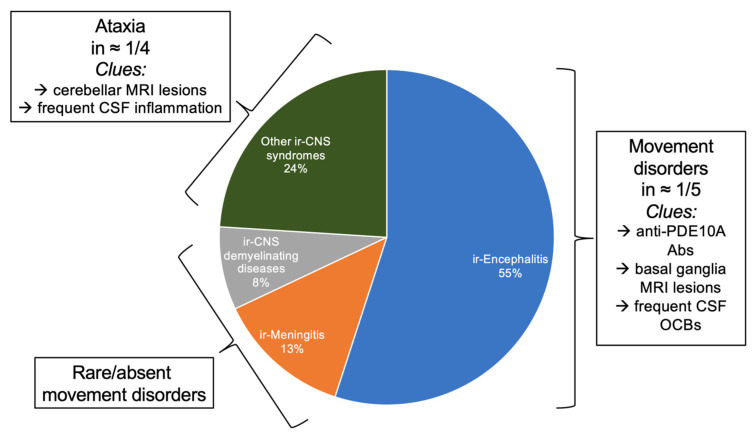
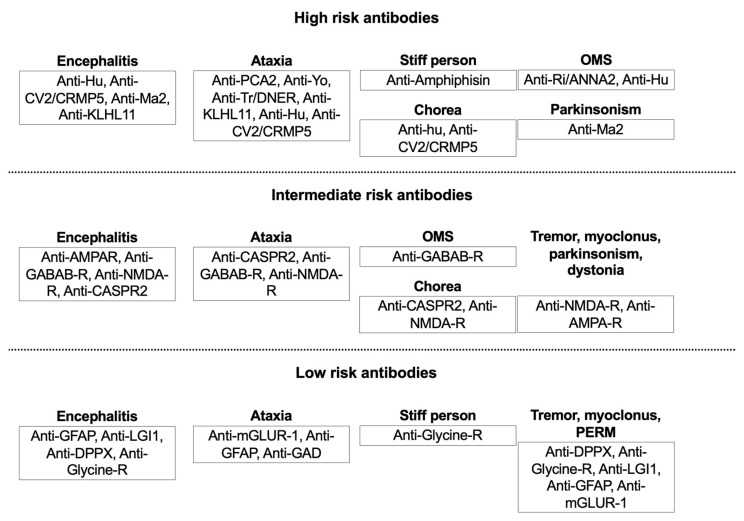
Results: movement disorders secondary to brain tumors are rare and may manifest with both hyper-/hypokinetic conditions. Paraneoplastic movement disorders are caused by antineuronal antibodies targeting intracellular or neuronal surface antigens, with variable prognosis and response to treatment. ICIs promote antitumor response by the inhibition of the immune checkpoints. They are effective treatments for several malignancies, but they may cause movement disorders through an unchecked immune response.
Conclusions: movement disorders due to focal neoplastic brain lesions are rare but should not be missed. Paraneoplastic movement disorders are even rarer, and their clinical-laboratory findings require focused expertise. In addition to their desired effects in cancer treatment, ICIs can induce specific neurological adverse events, sometimes manifesting with movement disorders, which often require a case-by-case, multidisciplinary, approach.
Keywords: autoimmune; immune-checkpoint inhibitors; movement disorders; oncology; paraneoplastic.
Conflict of interest statement
The authors declare no conflict of interest related to the present work.
Figures
References
-
- Hatano T.K.S., Hattori N., Mizuno Y. Movement disorders in neoplastic brain disease. In: W. Poewe J.J., editor. Movement Disorders in Neurologic and Systemic Disease. Cambridge University Press; Cambridge, UK: 2014. pp. 279–292.
Publication types
LinkOut - more resources
Full Text Sources
