

Neurogenic Inflammation: The Participant in Migraine and Recent Advancements in Translational Research
- PMID: 35052756
- PMCID: PMC8773152
- DOI: 10.3390/biomedicines10010076
Neurogenic Inflammation: The Participant in Migraine and Recent Advancements in Translational Research
Abstract
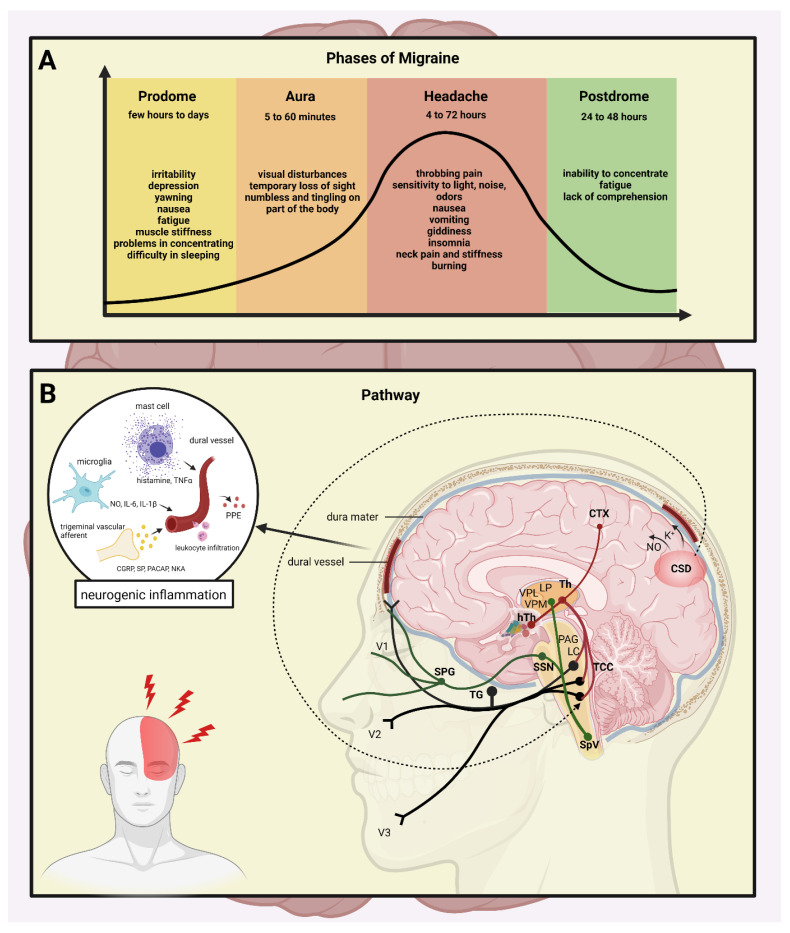
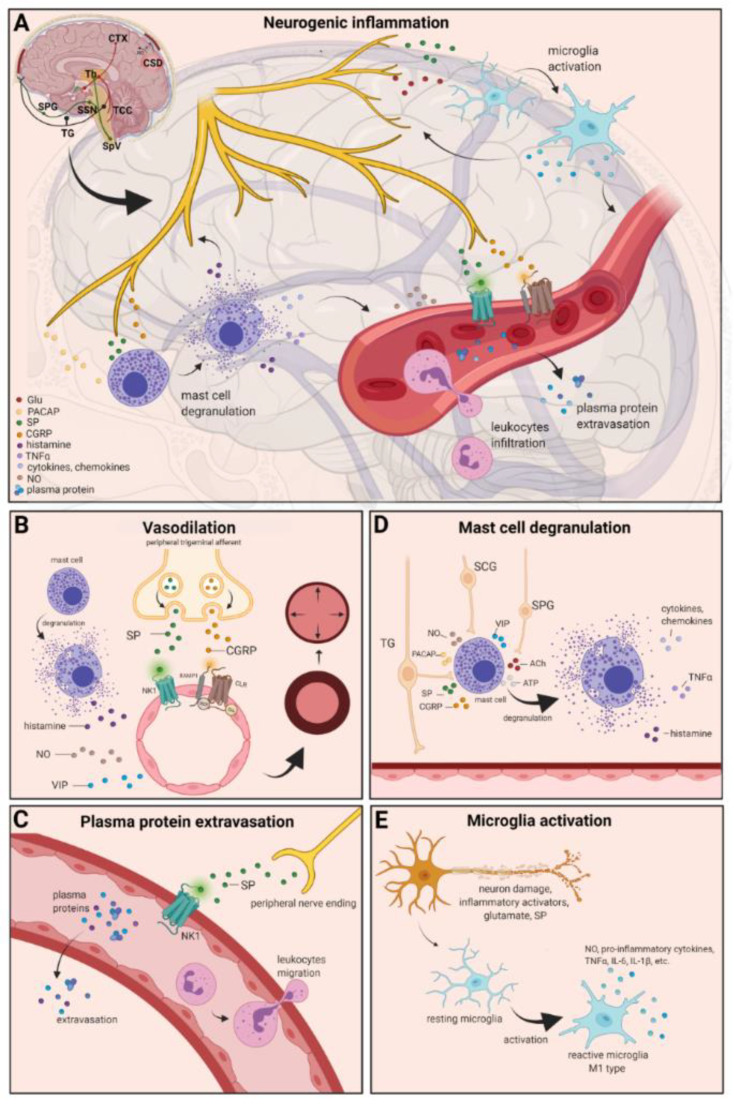
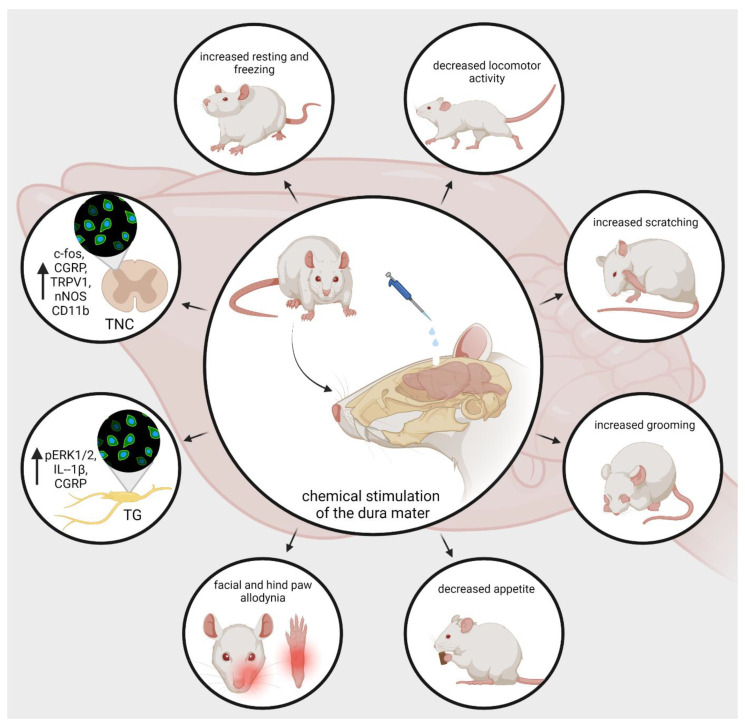
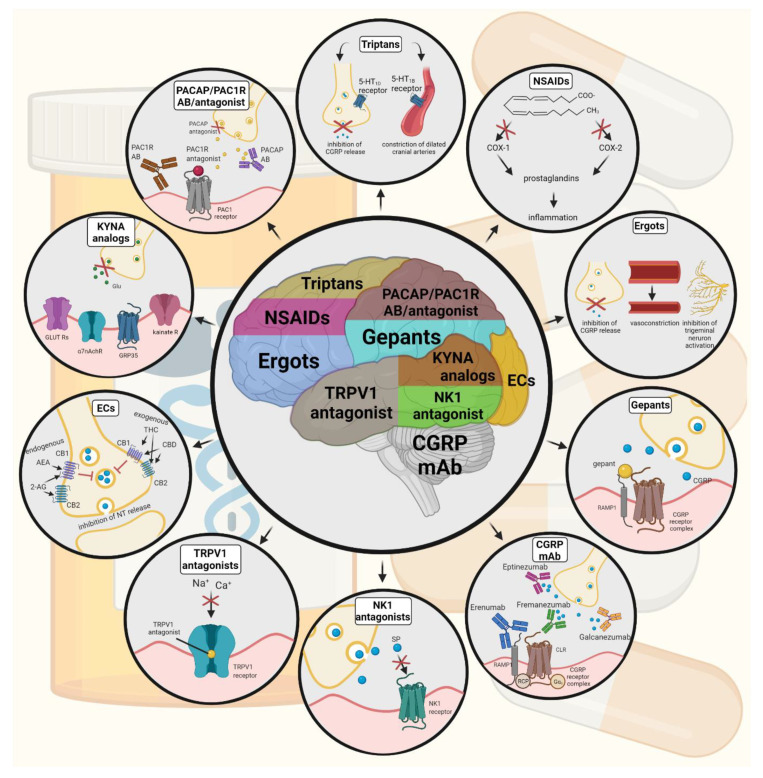
Migraine is a primary headache disorder characterized by a unilateral, throbbing, pulsing headache, which lasts for hours to days, and the pain can interfere with daily activities. It exhibits various symptoms, such as nausea, vomiting, sensitivity to light, sound, and odors, and physical activity consistently contributes to worsening pain. Despite the intensive research, little is still known about the pathomechanism of migraine. It is widely accepted that migraine involves activation and sensitization of the trigeminovascular system. It leads to the release of several pro-inflammatory neuropeptides and neurotransmitters and causes a cascade of inflammatory tissue responses, including vasodilation, plasma extravasation secondary to capillary leakage, edema, and mast cell degranulation. Convincing evidence obtained in rodent models suggests that neurogenic inflammation is assumed to contribute to the development of a migraine attack. Chemical stimulation of the dura mater triggers activation and sensitization of the trigeminal system and causes numerous molecular and behavioral changes; therefore, this is a relevant animal model of acute migraine. This narrative review discusses the emerging evidence supporting the involvement of neurogenic inflammation and neuropeptides in the pathophysiology of migraine, presenting the most recent advances in preclinical research and the novel therapeutic approaches to the disease.
Keywords: animal model; dura mater; immune system; inflammatory soup; migraine; migraine treatment; neurogenic inflammation; neuropeptides; primary headache; trigeminal system.
Conflict of interest statement
The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Figures
References
-
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390:1211–1259. doi: 10.1016/S0140-6736(17)32154-2. - DOI - PMC - PubMed
-
- Cerbo R., Pesare M., Aurilia C., Rondelli V., Barbanti P. Socio–economic costs of migraine. J. Headache Pain. 2001;2:s15–s19. doi: 10.1007/s101940170003. - DOI
-
- Mayans L., Walling A. Acute Migraine Headache: Treatment Strategies. Am. Fam. Physician. 2018;97:243–251. - PubMed
Publication types
Grants and funding
- GINOP 2.3.2-15-2016-00034/The Economic Development and Innovation Operational Programme (GINOP)
- GINOP 2.3.2-15-2016-00048/The Economic Development and Innovation Operational Programme (GINOP)
- NKFIH-1279-2/2020 TKP 2020/National Research, Development and Innovation Office
- TUDFO/47138-1/2019-ITM/TUDFO
- OTKA138125/National Scientific Research Fund (OTKA)
LinkOut - more resources
Full Text Sources
