

Definition of an Inflammatory Biomarker Signature in Plasma-Derived Extracellular Vesicles of Glioblastoma Patients
- PMID: 35052804
- PMCID: PMC8773644
- DOI: 10.3390/biomedicines10010125
Definition of an Inflammatory Biomarker Signature in Plasma-Derived Extracellular Vesicles of Glioblastoma Patients
Abstract
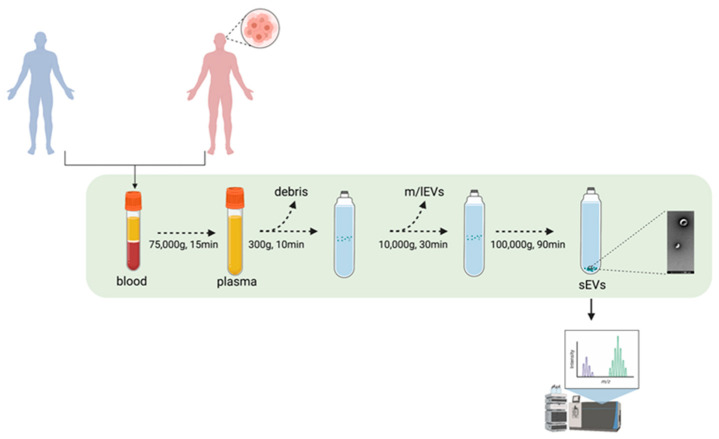
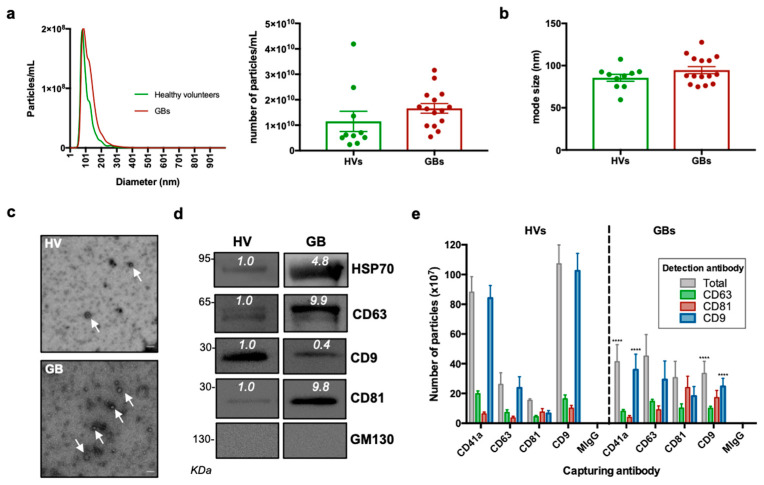
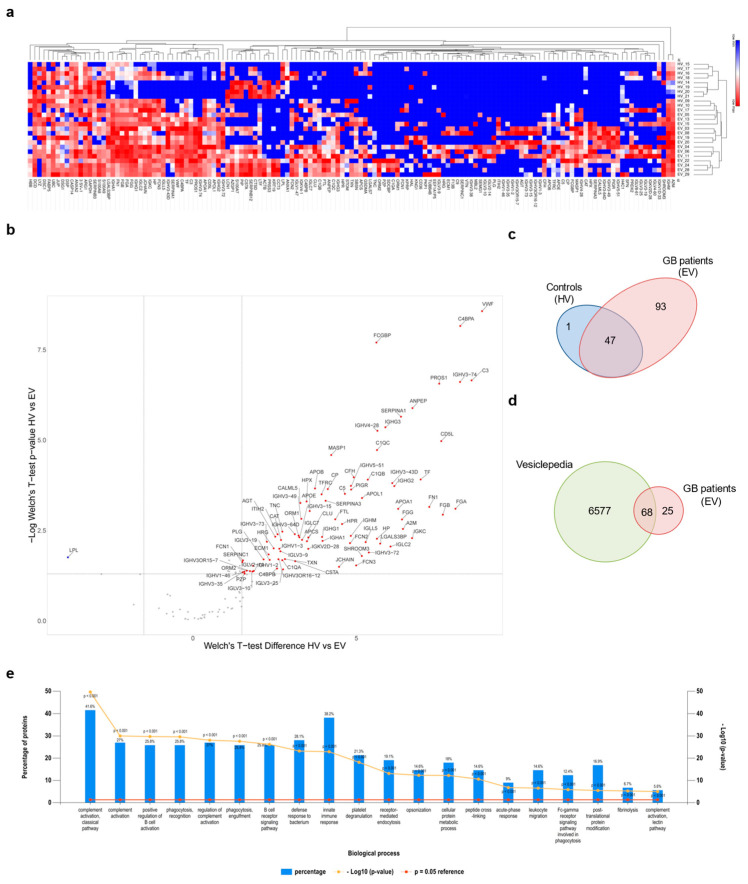
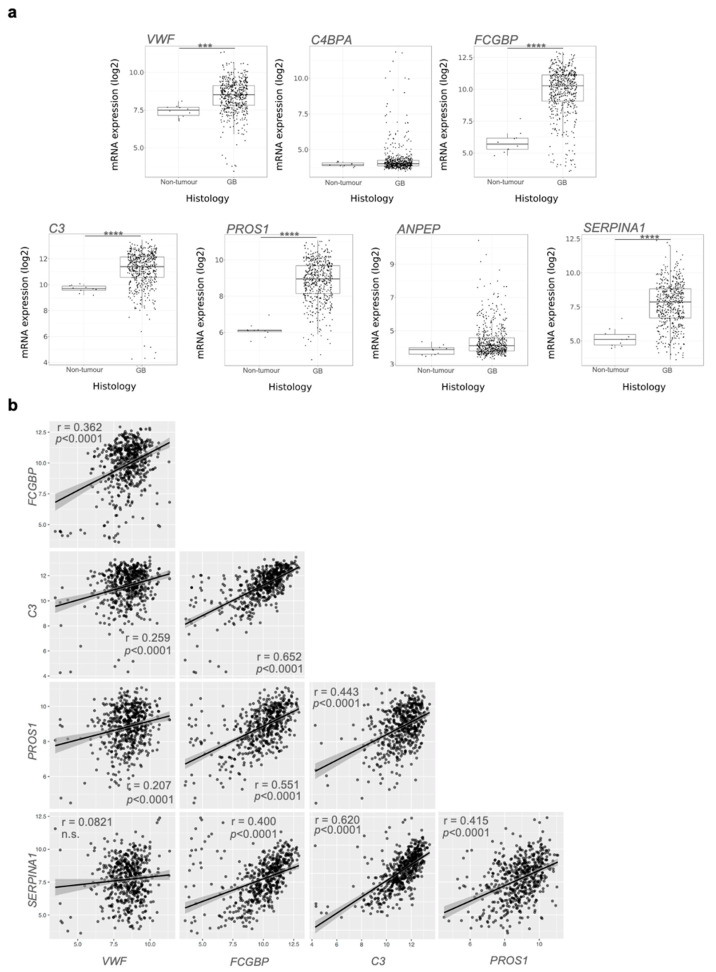
Glioblastoma (GB) is an aggressive type of tumour for which therapeutic options and biomarkers are limited. GB diagnosis mostly relies on symptomatic presentation of the tumour and, in turn, brain imaging and invasive biopsy that can delay its diagnosis. Description of easily accessible and effective biomarkers present in biofluids would thus prove invaluable in GB diagnosis. Extracellular vesicles (EVs) derived from both GB and stromal cells are essential to intercellular crosstalk in the tumour bulk, and circulating EVs have been described as a potential reservoir of GB biomarkers. Therefore, EV-based liquid biopsies have been suggested as a promising tool for GB diagnosis and follow up. To identify GB specific proteins, sEVs were isolated from plasma samples of GB patients as well as healthy volunteers using differential ultracentrifugation, and their content was characterised through mass spectrometry. Our data indicate the presence of an inflammatory biomarker signature comprising members of the complement and regulators of inflammation and coagulation including VWF, FCGBP, C3, PROS1, and SERPINA1. Overall, this study is a step forward in the development of a non-invasive liquid biopsy approach for the identification of valuable biomarkers that could significantly improve GB diagnosis and, consequently, patients' prognosis and quality of life.
Keywords: extracellular vesicles; glioblastoma; liquid biopsy.
Conflict of interest statement
Georgios Giamas is the Founder/Chief Scientific Officer of StingrayBio. No other conflicts are declared.
Figures
References
-
- Louis D.N., Perry A., Reifenberger G., von Deimling A., Figarella-Branger D., Cavenee W.K., Ohgaki H., Wiestler O.D., Kleihues P., Ellison D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016;131:803–820. doi: 10.1007/s00401-016-1545-1. - DOI - PubMed
-
- Louis D.N., Perry A., Wesseling P., Brat D.J., Cree I.A., Figarella-Branger D., Hawkins C., Ng H.K., Pfister S.M., Reifenberger G., et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro Oncol. 2021;23:1231–1251. doi: 10.1093/neuonc/noab106. - DOI - PMC - PubMed
-
- Verhaak R.G., Hoadley K.A., Purdom E., Wang V., Qi Y., Wilkerson M.D., Miller C.R., Ding L., Golub T., Mesirov J.P., et al. Integrated genomic analysis identifies clinically relevant subtypes of glioblastoma characterized by abnormalities in PDGFRA, IDH1, EGFR, and NF1. Cancer Cell. 2010;17:98–110. doi: 10.1016/j.ccr.2009.12.020. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
