

Analysis of Survival and Response to Lenvatinib in Unresectable Hepatocellular Carcinoma
- PMID: 35053484
- PMCID: PMC8774012
- DOI: 10.3390/cancers14020320
Analysis of Survival and Response to Lenvatinib in Unresectable Hepatocellular Carcinoma
Abstract
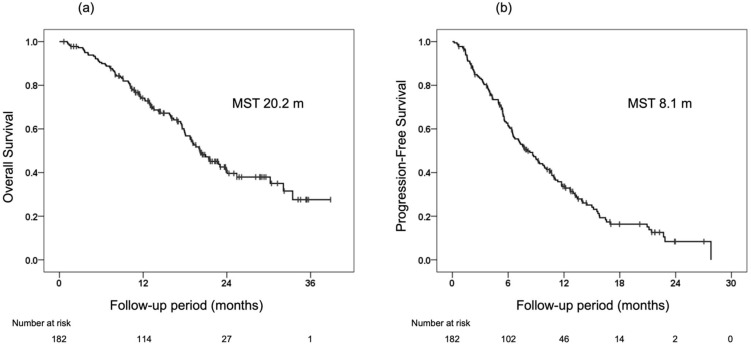
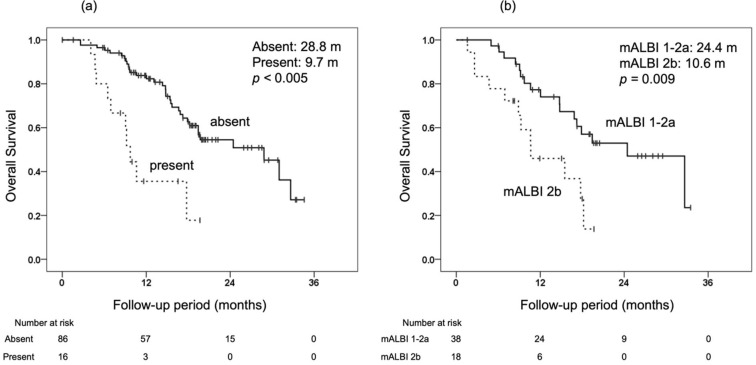
The association between radiological response and overall survival (OS) was retrospectively evaluated in patients treated with lenvatinib as a first-line systemic treatment for unresectable hepatocellular carcinoma. A total of 182 patients with Child-Pugh class A liver function and an Eastern Cooperative Oncology Group performance status of zero or one were enrolled. Radiological evaluation was performed using Response Evaluation Criteria in Solid Tumors (RECIST) and modified Response Evaluation Criteria in Solid Tumors (mRECIST). Initial radiological evaluation confirmed significant stratification of OS by efficacy judgment with both RECIST and mRECIST, and that initial radiological response was an independent prognostic factor for OS on multivariate analysis. Furthermore, in patients with stable disease (SD) at initial evaluation, macrovascular invasion at the initial evaluation on RECIST and modified albumin-bilirubin grade at initial evaluation on mRECIST were independent predictors of OS on multivariate analysis. In conclusion, if objective response is obtained at the initial evaluation, continuation of treatment appears desirable because prolonged OS can be expected; but, if SD is obtained at the initial evaluation, one should determine whether to continue or switch to the next treatment, with careful consideration of factors related to the tumor and hepatic reserve at the initial evaluation.
Keywords: Response Evaluation Criteria in Solid Tumors (RECIST); hepatocellular carcinoma; lenvatinib; modified Response Evaluation Criteria in Solid Tumors (mRECIST); molecular targeted agent; overall survival; radiological response; sequential therapy.
Conflict of interest statement
M. I. has received research funding from Bristol Myers Squibb and AbbVie. H. A. has received honoraria from Eisai and Bayer. The other authors declare no conflicts of interest.
Figures

References
-
- Llovet J.M., Real M.I., Montaña X., Planas R., Coll S., Aponte J., Ayuso C., Sala M., Muchart J., Sola R., et al. Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: A randomised controlled trial. Lancet. 2002;359:1734–1739. doi: 10.1016/S0140-6736(02)08649-X. - DOI - PubMed
-
- Obi S., Yoshida H., Toune R., Unuma T., Kanda M., Sato S., Tateishi R., Teratani T., Shiina S., Omata M. Combination therapy of intra-arterial 5-fluorouracil and systemic interferon-alpha for advanced hepatocellular carcinoma with portal venous invasion. Cancer. 2006;106:1990–1997. doi: 10.1002/cncr.21832. - DOI - PubMed
LinkOut - more resources
Full Text Sources
