

Klotho and Mesenchymal Stem Cells: A Review on Cell and Gene Therapy for Chronic Kidney Disease and Acute Kidney Disease
- PMID: 35056905
- PMCID: PMC8778857
- DOI: 10.3390/pharmaceutics14010011
Klotho and Mesenchymal Stem Cells: A Review on Cell and Gene Therapy for Chronic Kidney Disease and Acute Kidney Disease
Abstract
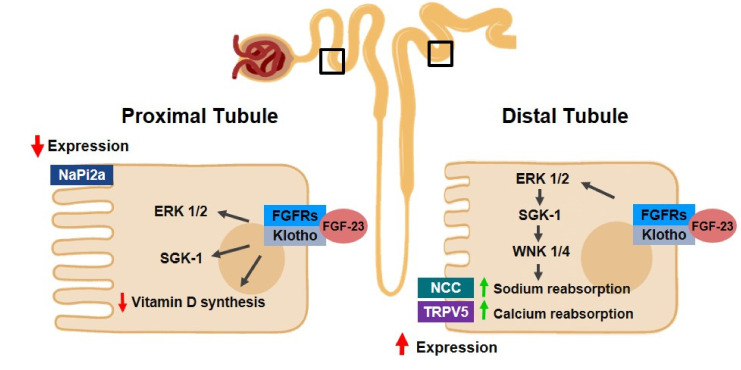
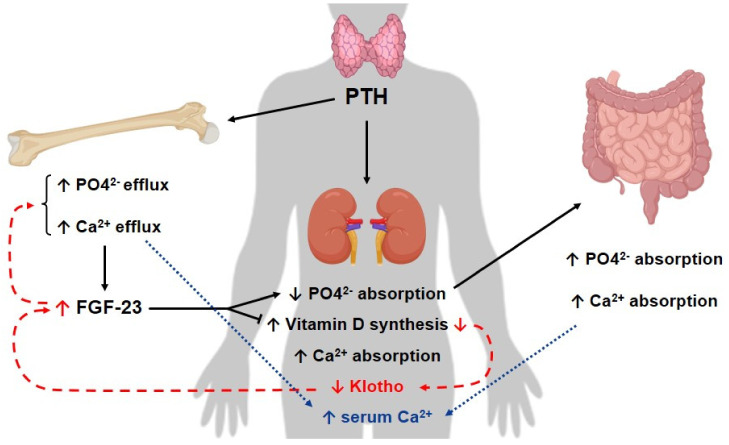
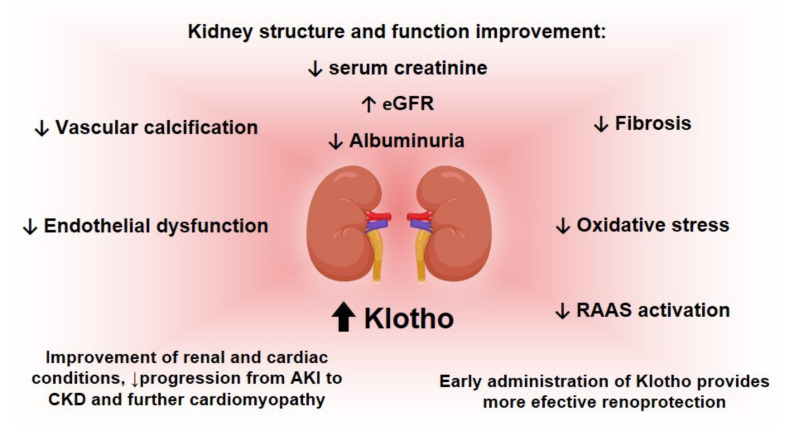
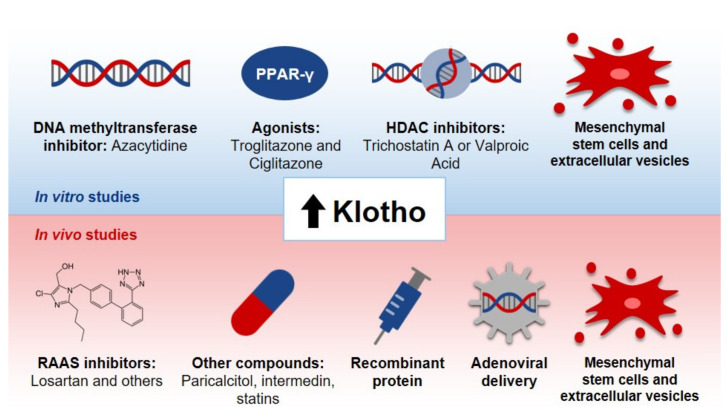
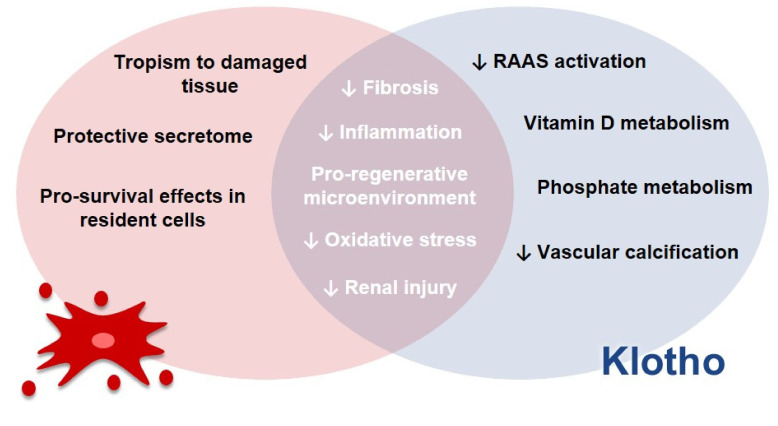
Chronic kidney disease (CKD) and acute kidney injury (AKI) are public health problems, and their prevalence rates have increased with the aging of the population. They are associated with the presence of comorbidities, in particular diabetes mellitus and hypertension, resulting in a high financial burden for the health system. Studies have indicated Klotho as a promising therapeutic approach for these conditions. Klotho reduces inflammation, oxidative stress and fibrosis and counter-regulates the renin-angiotensin-aldosterone system. In CKD and AKI, Klotho expression is downregulated from early stages and correlates with disease progression. Therefore, the restoration of its levels, through exogenous or endogenous pathways, has renoprotective effects. An important strategy for administering Klotho is through mesenchymal stem cells (MSCs). In summary, this review comprises in vitro and in vivo studies on the therapeutic potential of Klotho for the treatment of CKD and AKI through the administration of MSCs.
Keywords: Klotho; acute kidney injury; chronic kidney disease; mesenchymal stem cells.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
