

Spatiotemporal prediction of vancomycin-resistant Enterococcus colonisation
- PMID: 35057734
- PMCID: PMC8781237
- DOI: 10.1186/s12879-022-07043-9
Spatiotemporal prediction of vancomycin-resistant Enterococcus colonisation
Abstract
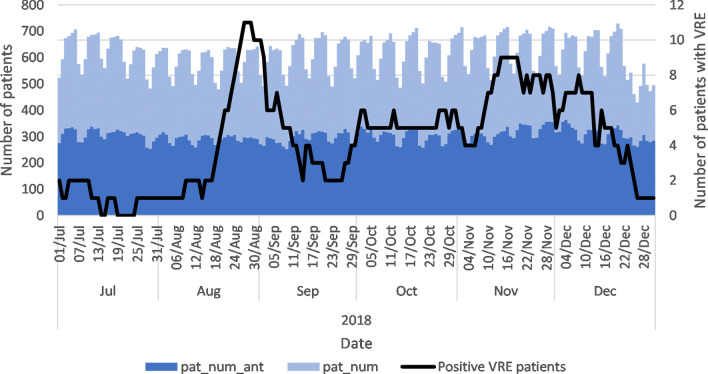
Background: Vancomycin-resistant enterococci (VRE) is the cause of severe patient health and monetary burdens. Antibiotic use is a confounding effect to predict VRE in patients, but the antibiotic use of patients who may have frequented the same ward as the patient in question is often neglected. This study investigates how patient movements between hospital wards and their antibiotic use can explain the colonisation of patients with VRE.
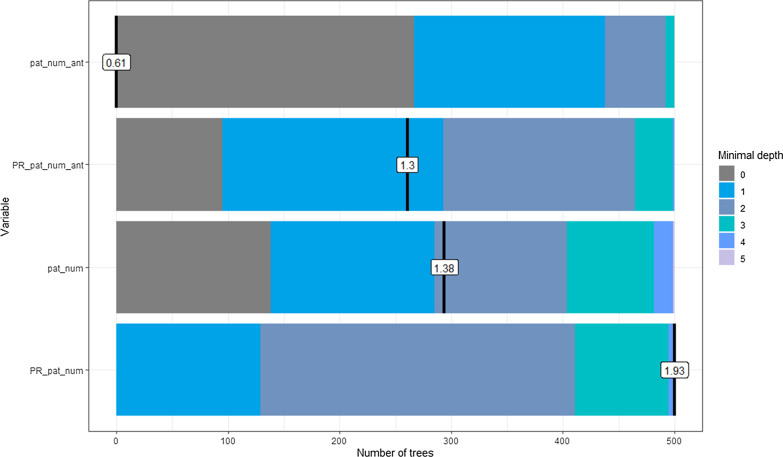
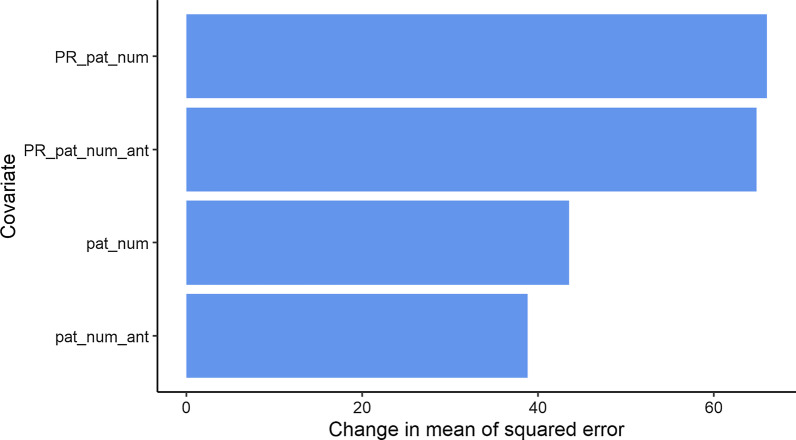
Methods: Intrahospital patient movements, antibiotic use and PCR screening data were used from a hospital in the Netherlands. The PageRank algorithm was used to calculate two daily centrality measures based on the spatiotemporal graph to summarise the flow of patients and antibiotics at the ward level. A decision tree model was used to determine a simple set of rules to estimate the daily probability of patient VRE colonisation for each hospital ward. The model performance was improved using a random forest model and compared using 30% test sample.
Results: Centrality covariates summarising the flow of patients and their antibiotic use between hospital wards can be used to predict the daily colonisation of VRE at the hospital ward level. The decision tree model produced a simple set of rules that can be used to determine the daily probability of patient VRE colonisation for each hospital ward. An acceptable area under the ROC curve (AUC) of 0.755 was achieved using the decision tree model and an excellent AUC of 0.883 by the random forest model on the test set. These results confirms that the random forest model performs better than a single decision tree for all levels of model sensitivity and specificity on data not used to estimate the models.
Conclusion: This study showed how the movements of patients inside hospitals and their use of antibiotics could predict the colonisation of patients with VRE at the ward level. Two daily centrality measures were proposed to summarise the flow of patients and antibiotics at the ward level. An early warning system for VRE can be developed to test and further develop infection prevention plans and outbreak strategies using these results.
Keywords: Centrality measure; Dynamic directed spatiotemporal graph; Healthcare decision support; Intrahospital patient movements; Spatiotemporal risk factors; Vancomycin-resistant enterococci.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they do not have any conflict of interest.
Figures







References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
