

Comparison of statistical methods for the analysis of recurrent adverse events in the presence of non-proportional hazards and unobserved heterogeneity: a simulation study
- PMID: 35057743
- PMCID: PMC8771190
- DOI: 10.1186/s12874-021-01475-8
Comparison of statistical methods for the analysis of recurrent adverse events in the presence of non-proportional hazards and unobserved heterogeneity: a simulation study
Abstract
Background: In preventive drug trials such as intermittent preventive treatment for malaria prevention during pregnancy (IPTp), where there is repeated treatment administration, recurrence of adverse events (AEs) is expected. Challenges in modelling the risk of the AEs include accounting for time-to-AE and within-patient-correlation, beyond the conventional methods. The correlation comes from two sources; (a) individual patient unobserved heterogeneity (i.e. frailty) and (b) the dependence between AEs characterised by time-dependent treatment effects. Potential AE-dependence can be modelled via time-dependent treatment effects, event-specific baseline and event-specific random effect, while heterogeneity can be modelled via subject-specific random effect. Methods that can improve the estimation of both the unobserved heterogeneity and treatment effects can be useful in understanding the evolution of risk of AEs, especially in preventive trials where time-dependent treatment effect is expected.
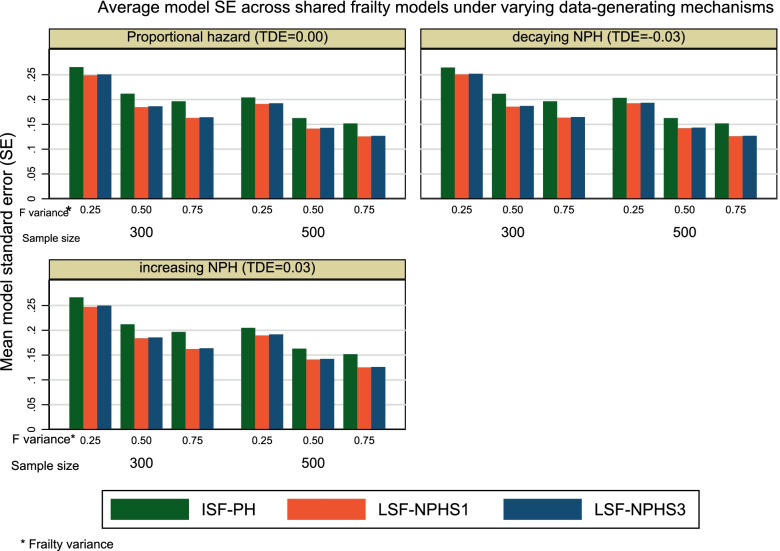
Methods: Using both a simulation study and the Chloroquine for Malaria in Pregnancy (NCT01443130) trial data to demonstrate the application of the models, we investigated whether the lognormal shared frailty models with restricted cubic splines and non-proportional hazards (LSF-NPH) assumption can improve estimates for both frailty variance and treatment effect compared to the conventional inverse Gaussian shared frailty model with proportional hazard (ISF-PH), in the presence of time-dependent treatment effects and unobserved patient heterogeneity. We assessed the bias, precision gain and coverage probability of 95% confidence interval of the frailty variance estimates for the models under varying known unobserved heterogeneity, sample sizes and time-dependent effects.
Results: The ISF-PH model provided a better coverage probability of 95% confidence interval, less bias and less precise frailty variance estimates compared to the LSF-NPH models. The LSF-NPH models yielded unbiased hazard ratio estimates at the expense of imprecision and high mean square error compared to the ISF-PH model.
Conclusion: The choice of the shared frailty model for the recurrent AEs analysis should be driven by the study objective. Using the LSF-NPH models is appropriate if unbiased hazard ratio estimation is of primary interest in the presence of time-dependent treatment effects. However, ISF-PH model is appropriate if unbiased frailty variance estimation is of primary interest.
Trial registration: ClinicalTrials.gov; NCT01443130.
Keywords: Non-proportional hazards; Randomised controlled trials; Recurrent adverse events; Unobserved heterogeneity.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Munsaka MS. Biopharmaceutical Applied Statistics Symposium. Biostatistical analysis of clinical trials, Vol. 2. Singapore: Springer; 2018. A question-based approach to the analysis of safety data; pp. 193–216.
-
- Phillips R, Cornelius V. Understanding current practice, identifying barriers and exploring priorities for adverse event analysis in randomised controlled trials: an online, cross-sectional survey of statisticians from academia and industry. BMJ Open. 2020;10(6):e036875. doi: 10.1136/bmjopen-2020-036875. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
