

Stroke in Takayasu arteritis with concomitant tuberculosis: an unusual pediatric case report
- PMID: 35057771
- PMCID: PMC8772212
- DOI: 10.1186/s12887-022-03125-4
Stroke in Takayasu arteritis with concomitant tuberculosis: an unusual pediatric case report
Abstract
Background: Stroke is a lethal complication of polyarteritis in children. Takayasu arteritis is a rare disease with an unknown etiology and is known to mainly affect young women. In this report, we present the case of a Chinese boy diagnosed with TA results in stroke, originally presenting in the context of latent tuberculosis infection and then developing active tuberculosis.
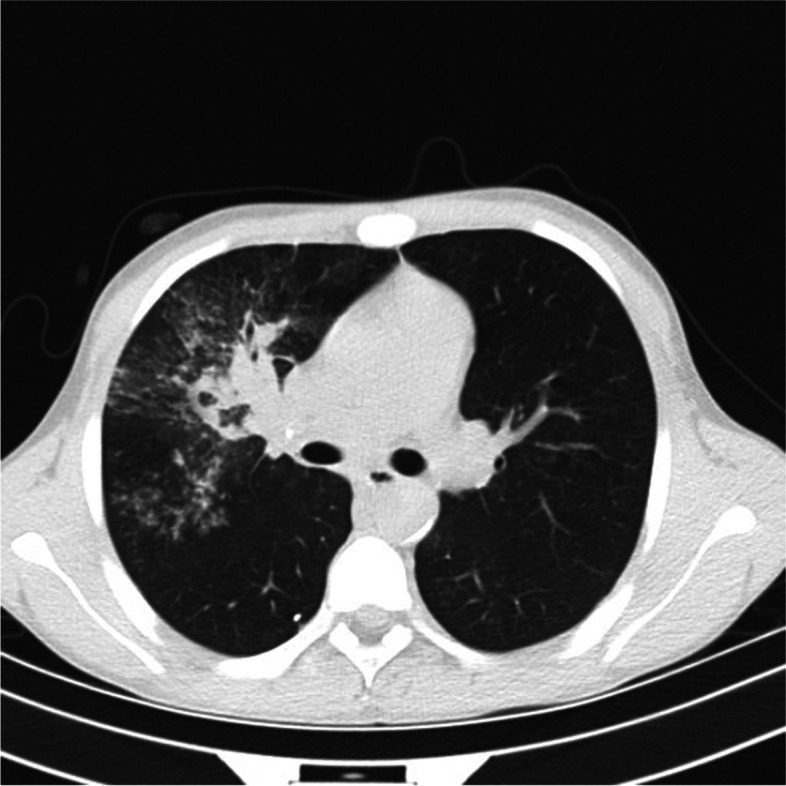
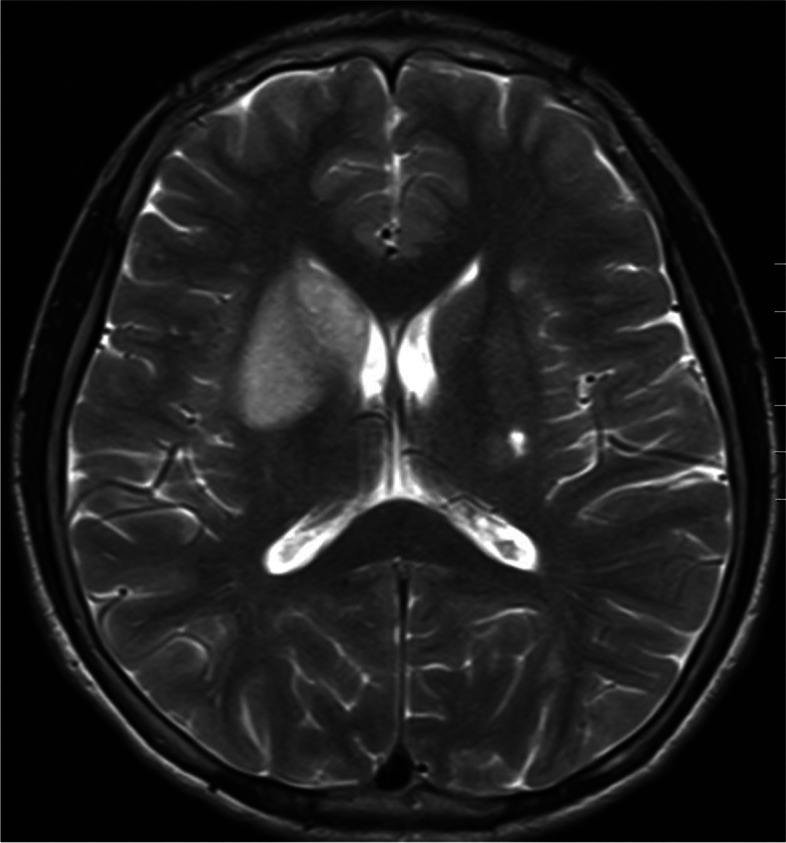
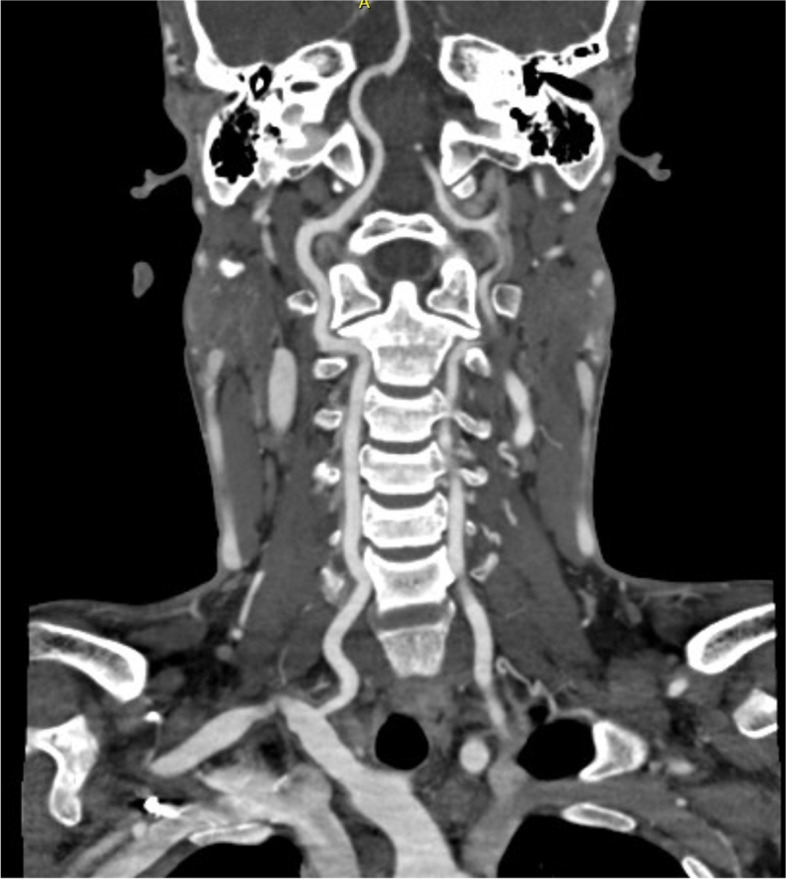
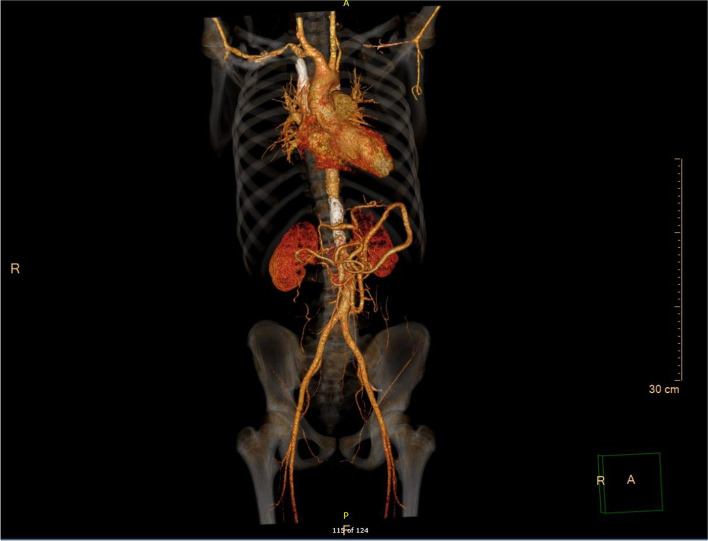
Case presentation: The patient was a 14-year-old child who developed a latent tuberculosis infection at age 5 after coming in close contact with his grandfather, who had tuberculosis. However, he did not receive any anti-tuberculosis medications at that time. At age 9, he was hospitalized for symptoms of "dizziness and headache" and was diagnosed with Takayasu arteritis and hypertension; however, tuberculosis was not diagnosed. Only antihypertensive drugs were administered without considering the possible pathogenic factors of tuberculosis infection. At age 14, he was rehospitalized for "fever and cough" and was diagnosed with active pulmonary tuberculosis as an analysis of his fiberoptic bronchoscopy sample using the Gene-Xpert assay was positive for Mycobacterium tuberculosis. However, after 2 months of taking oral anti-tuberculosis drugs, his blood pressure continued to rise, and he presented with numbness and weakness of the right limb and a deviation of the right side of his mouth. Computed tomography angiography of his head and neck revealed that the walls of the left subclavian artery and bilateral vertebral arteries were thickened, and the lumen was significantly narrowed. In a recent examination, magnetic resonance imaging and diffusion-weighted imaging of the head showed infarctions in the right basal ganglia area close to the left lateral ventricle. Our patient was treated with methotrexate, tocilizumab and glucocorticoids to control he continued active vasculitis.
Conclusions: The possible association of tuberculosis and Takayasu arteritis complicated by stroke needs to be considered, especially in children who had prior contact with a family member with tuberculosis infection. The temporal relationship between TA and infection with Mycobacterium tuberculosis in our patient suggests a compelling link that demands further investigation.
Keywords: Case report; Child; Mycobacterium tuberculosis; Stroke; Takayasu arteritis.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
