

Humoral immune response after different SARS-CoV-2 vaccination regimens
- PMID: 35057798
- PMCID: PMC8776512
- DOI: 10.1186/s12916-021-02231-x
Humoral immune response after different SARS-CoV-2 vaccination regimens
Abstract
Background: The humoral immune response after primary immunisation with a SARS-CoV-2 vector vaccine (AstraZeneca AZD1222, ChAdOx1 nCoV-19, Vaxzevria) followed by an mRNA vaccine boost (Pfizer/BioNTech, BNT162b2; Moderna, m-1273) was examined and compared with the antibody response after homologous vaccination schemes (AZD1222/AZD1222 or BNT162b2/BNT162b2).
Methods: Sera from 59 vaccinees were tested for anti-SARS-CoV-2 immunoglobulin G (IgG) and virus-neutralising antibodies (VNA) with three IgG assays based on (parts of) the SARS-CoV-2 spike (S)-protein as antigen, an IgG immunoblot (additionally contains the SARS-CoV-2 nucleoprotein (NP) as an antigen), a surrogate neutralisation test (sVNT), and a Vero-cell-based virus-neutralisation test (cVNT) with the B.1.1.7 variant of concern (VOC; alpha) as antigen. Investigation was done before and after heterologous (n = 30 and 42) or homologous booster vaccination (AZD1222/AZD1222, n = 8/9; BNT162b2/BNT162b2, n = 8/8). After the second immunisation, a subgroup of 26 age- and gender-matched sera (AZD1222/mRNA, n = 9; AZD1222/AZD1222, n = 9; BNT162b2/BNT162b2, n = 8) was also tested for VNA against VOC B.1.617.2 (delta) in the cVNT. The strength of IgG binding to separate SARS-CoV-2 antigens was measured by avidity.
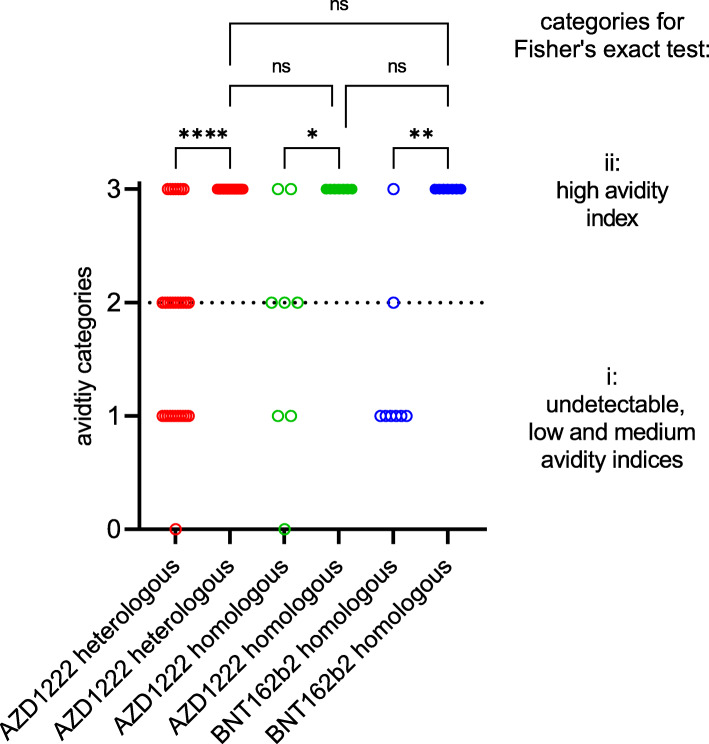
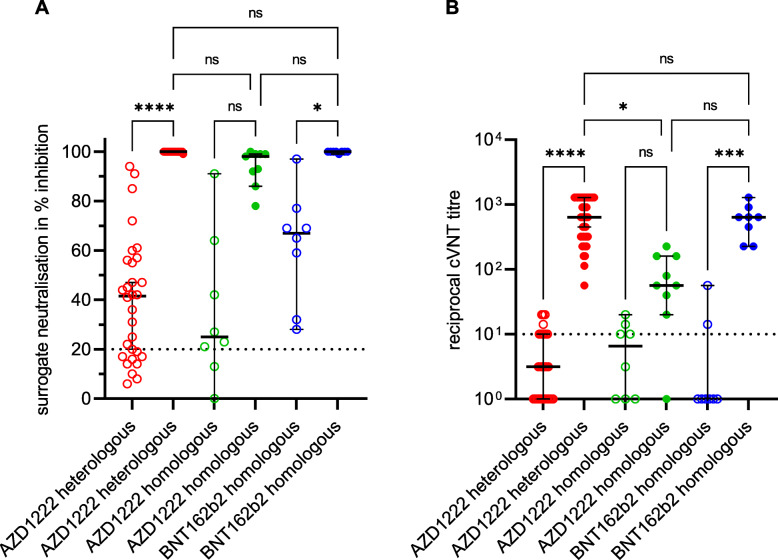
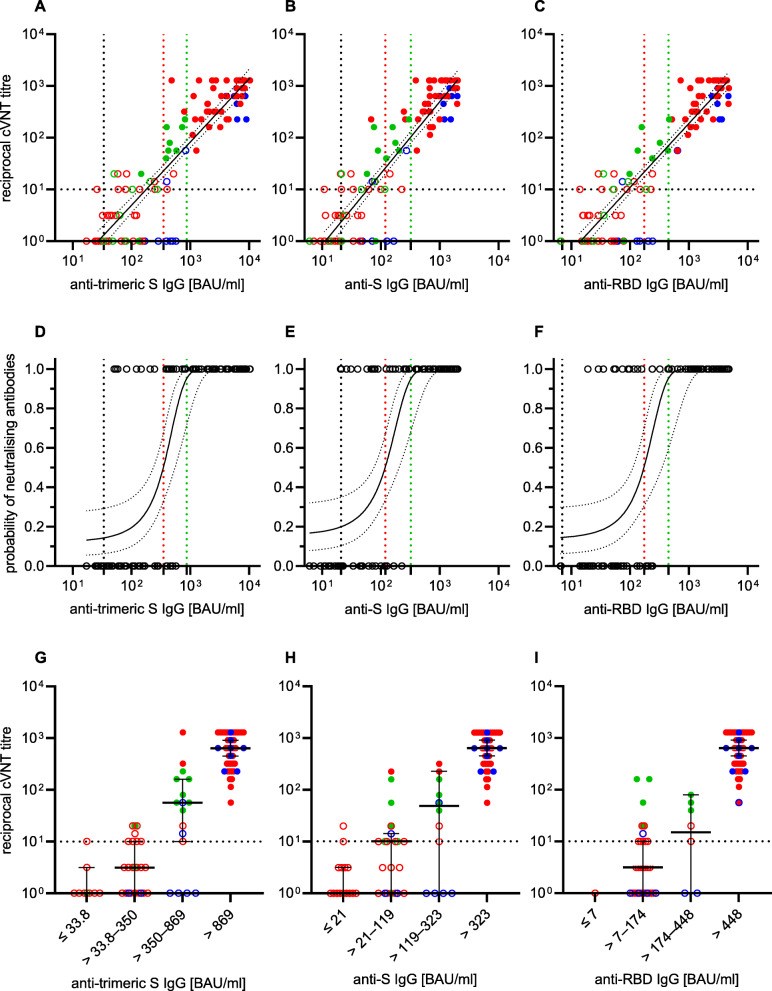
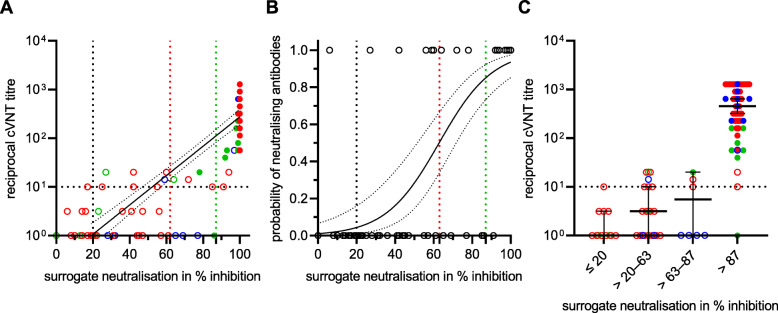
Results: After the first vaccination, the prevalence of IgG directed against the (trimeric) SARS-CoV-2 S-protein and its receptor binding domain (RBD) varied from 55-95% (AZD1222) to 100% (BNT162b2), depending on the vaccine regimen and the SARS-CoV-2 antigen used. The booster vaccination resulted in 100% seroconversion and the occurrence of highly avid IgG, which is directed against the S-protein subunit 1 and the RBD, as well as VNA against VOC B.1.1.7, while anti-NP IgGs were not detected. The results of the three anti-SARS-CoV-2 IgG tests showed an excellent correlation to the VNA titres against this VOC. The agreement of cVNT and sVNT results was good. However, the sVNT seems to overestimate non- and weak B.1.1.7-neutralising titres. The anti-SARS-CoV-2 IgG concentrations and the B.1.1.7-neutralising titres were significantly higher after heterologous vaccination compared to the homologous AZD1222 scheme. If VOC B.1.617.2 was used as antigen, significantly lower VNA titres were measured in the cVNT, and three (33.3%) vector vaccine recipients had a VNA titre < 1:10.
Conclusions: Heterologous SARS-CoV-2 vaccination leads to a strong antibody response with anti-SARS-CoV-2 IgG concentrations and VNA titres at a level comparable to that of a homologous BNT162b2 vaccination scheme. Irrespective of the chosen immunisation regime, highly avid IgG antibodies can be detected just 2 weeks after the second vaccine dose indicating the development of a robust humoral immunity. The reduction in the VNA titre against VOC B.1.617.2 observed in the subgroup of 26 individuals is remarkable and confirms the immune escape of the delta variant.
Keywords: COVID-19; Immunoglobulin G; Maturity process; Vaccination schemes; Virus neutralisation; Virus variants of concern.
© 2022. The Author(s).
Conflict of interest statement
The companies Abbott GmbH, Diasorin GmbH, Mikrogen GmbH and Tecomedical GmbH supported this study by providing free or discounted kits. None of the four companies had any influence on the testing and the interpretation of the results. The authors declare that they have no competing interests.
Figures


References
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
