

Robotic surgery in emergency setting: 2021 WSES position paper
- PMID: 35057836
- PMCID: PMC8781145
- DOI: 10.1186/s13017-022-00410-6
Robotic surgery in emergency setting: 2021 WSES position paper
Abstract
Background: Robotics represents the most technologically advanced approach in minimally invasive surgery (MIS). Its application in general surgery has increased progressively, with some early experience reported in emergency settings. The present position paper, supported by the World Society of Emergency Surgery (WSES), aims to provide a systematic review of the literature to develop consensus statements about the potential use of robotics in emergency general surgery.
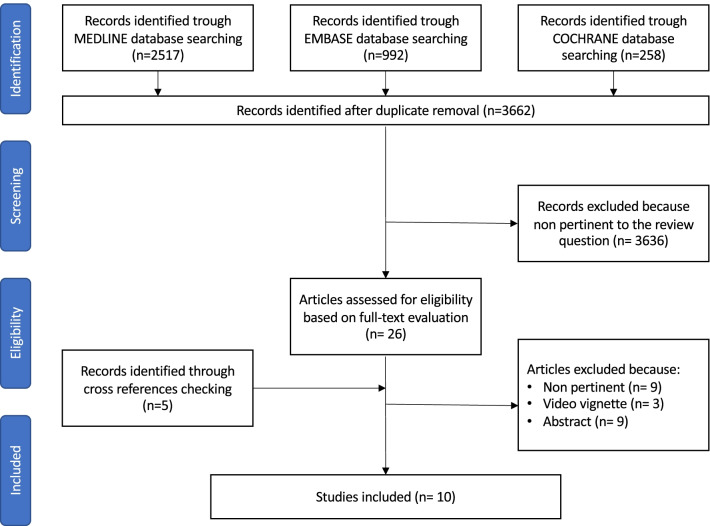
Methods: This position paper was conducted according to the WSES methodology. A steering committee was constituted to draft the position paper according to the literature review. An international expert panel then critically revised the manuscript. Each statement was voted through a web survey to reach a consensus.
Results: Ten studies (3 case reports, 3 case series, and 4 retrospective comparative cohort studies) have been published regarding the applications of robotics for emergency general surgery procedures. Due to the paucity and overall low quality of evidence, 6 statements are proposed as expert opinions. In general, the experts claim for a strict patient selection while approaching emergent general surgery procedures with robotics, eventually considering it for hemodynamically stable patients only. An emergency setting should not be seen as an absolute contraindication for robotic surgery if an adequate training of the operating surgical team is available. In such conditions, robotic surgery can be considered safe, feasible, and associated with surgical outcomes related to an MIS approach. However, there are some concerns regarding the adoption of robotic surgery for emergency surgeries associated with the following: (i) the availability and accessibility of the robotic platform for emergency units and during night shifts, (ii) expected longer operative times, and (iii) increased costs. Further research is necessary to investigate the role of robotic surgery in emergency settings and to explore the possibility of performing telementoring and telesurgery, which are particularly valuable in emergency situations.
Conclusions: Many hospitals are currently equipped with a robotic surgical platform which needs to be implemented efficiently. The role of robotic surgery for emergency procedures remains under investigation. However, its use is expanding with a careful assessment of costs and timeliness of operations. The proposed statements should be seen as a preliminary guide for the surgical community stressing the need for reevaluation and update processes as evidence expands in the relevant literature.
Keywords: Emergency surgery; General surgery; Minimally invasive surgery; Robotic surgery.
© 2022. The Author(s).
Conflict of interest statement
P Pessaux declared that he received consulting fees from 3M and Integra and has stock-options of Virtualisurg. E Kouwenhoven is proctor for Intuitive Surgical. M Sugrue received consulting fee with 3M, Smith and Nephew and Novus Scientific. G Spinoglio received honoraria as proctor for Intuitive Surgical. F. Ris reports research funding from Quantgene, personal fees from Arthrex, Stryker, Hollister, Fresenius Kabi and Distal Motion, outside the submitted work. E Espin Bsany received honoraria as proctor for Intuitive Surgical. JS Khan is a proctor for Intuitive Surgical. All other authors have no conflicts of interest to declare in relation to the matter of this publication.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
