

Lifetime Risk of Heart Failure Among Participants in the Framingham Study
- PMID: 35057911
- PMCID: PMC8820638
- DOI: 10.1016/j.jacc.2021.10.043
Lifetime Risk of Heart Failure Among Participants in the Framingham Study
Abstract
Background: The residual lifetime risk (RLR) of developing heart failure (HF) may have changed over time because of the increasing population burden of hypertension, obesity, and diabetes; greater survival after myocardial infarction; and a greater lifespan.
Objectives: The authors assessed changes in the RLR for HF in two 25-year epochs (1965-1989 and 1990-2014).
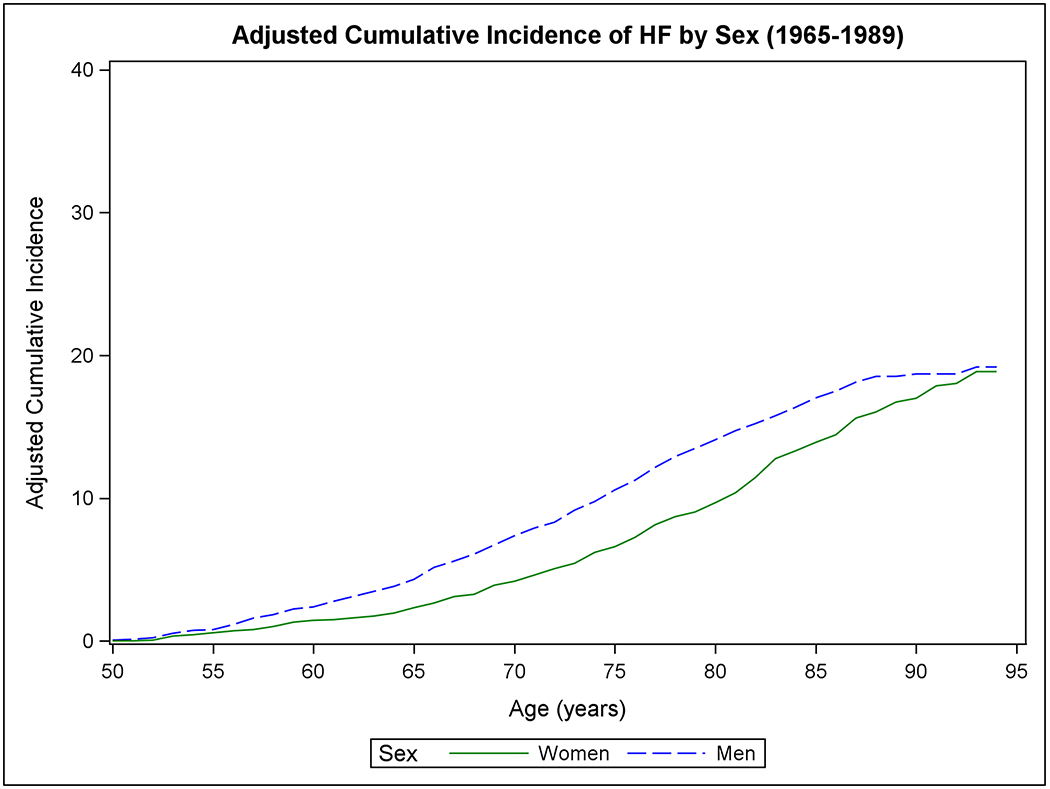
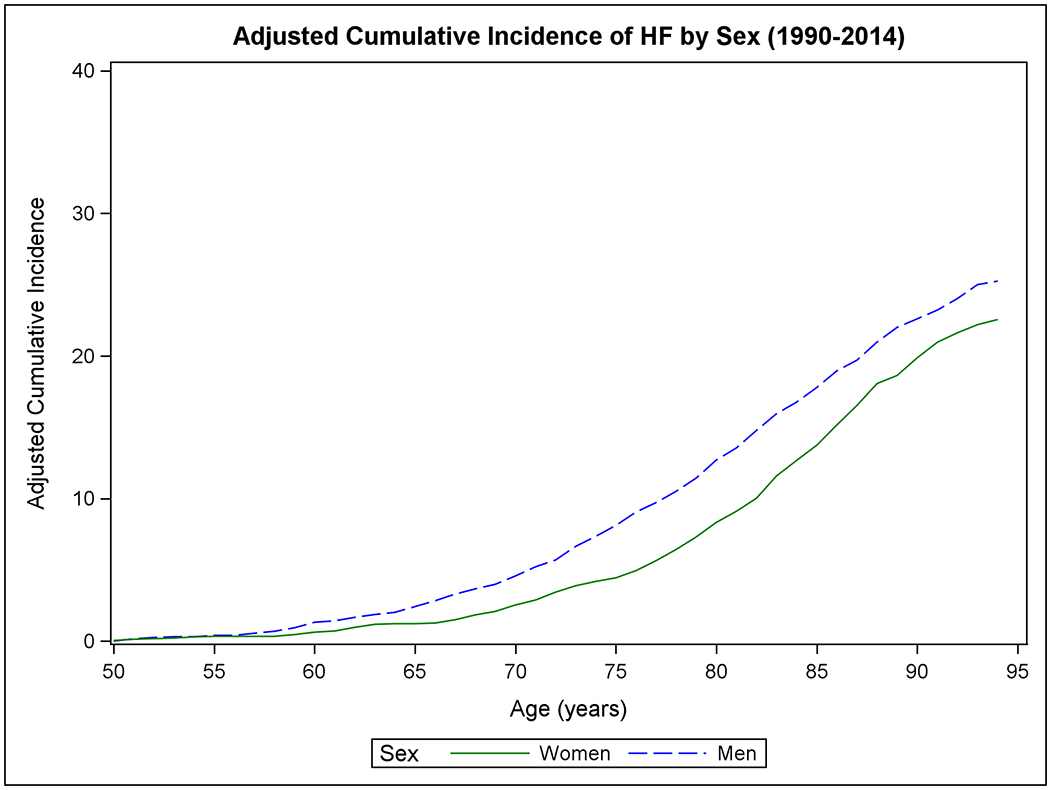
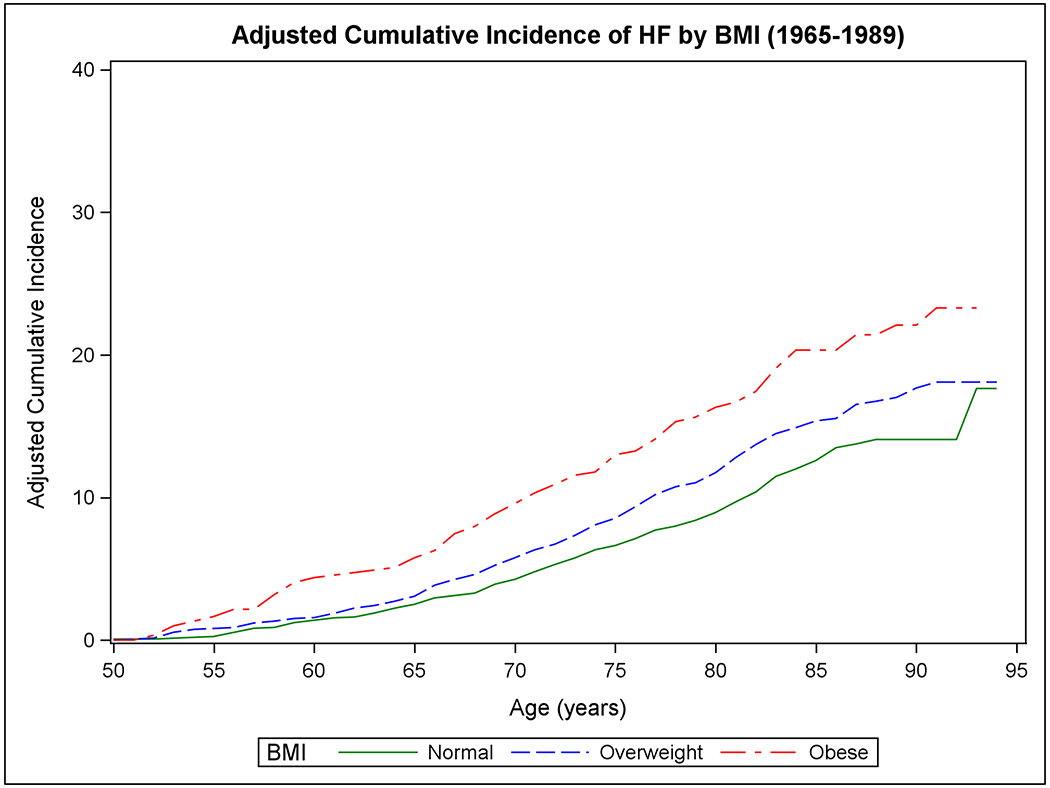
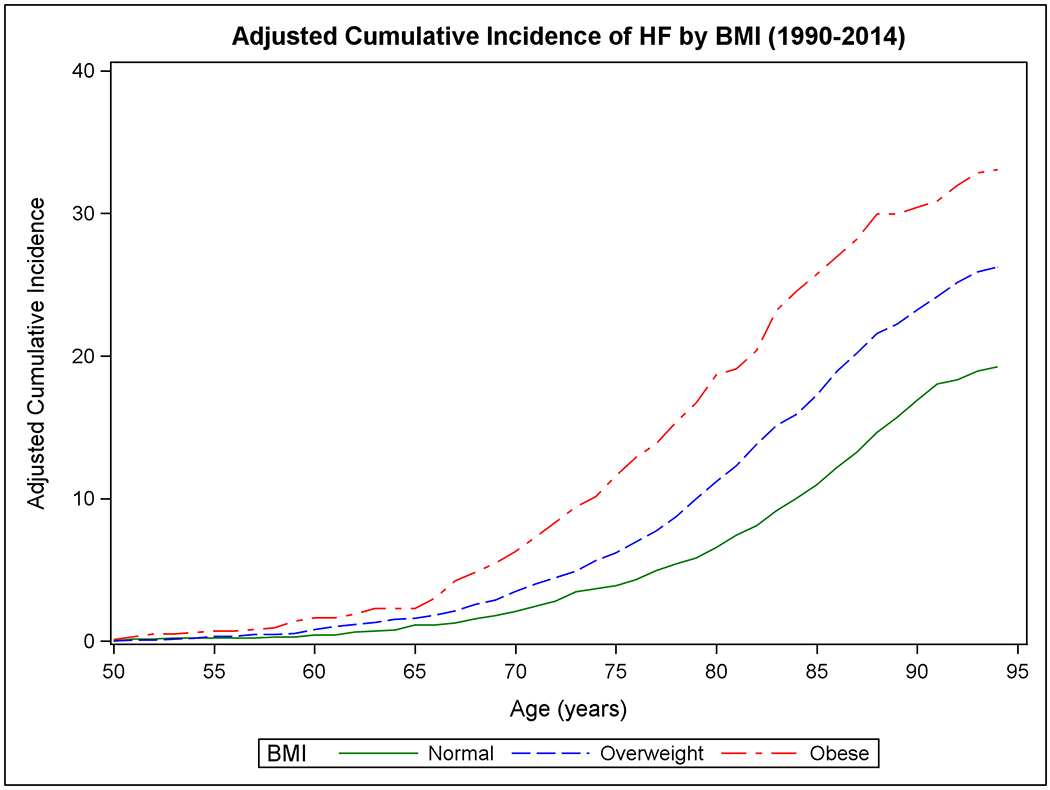
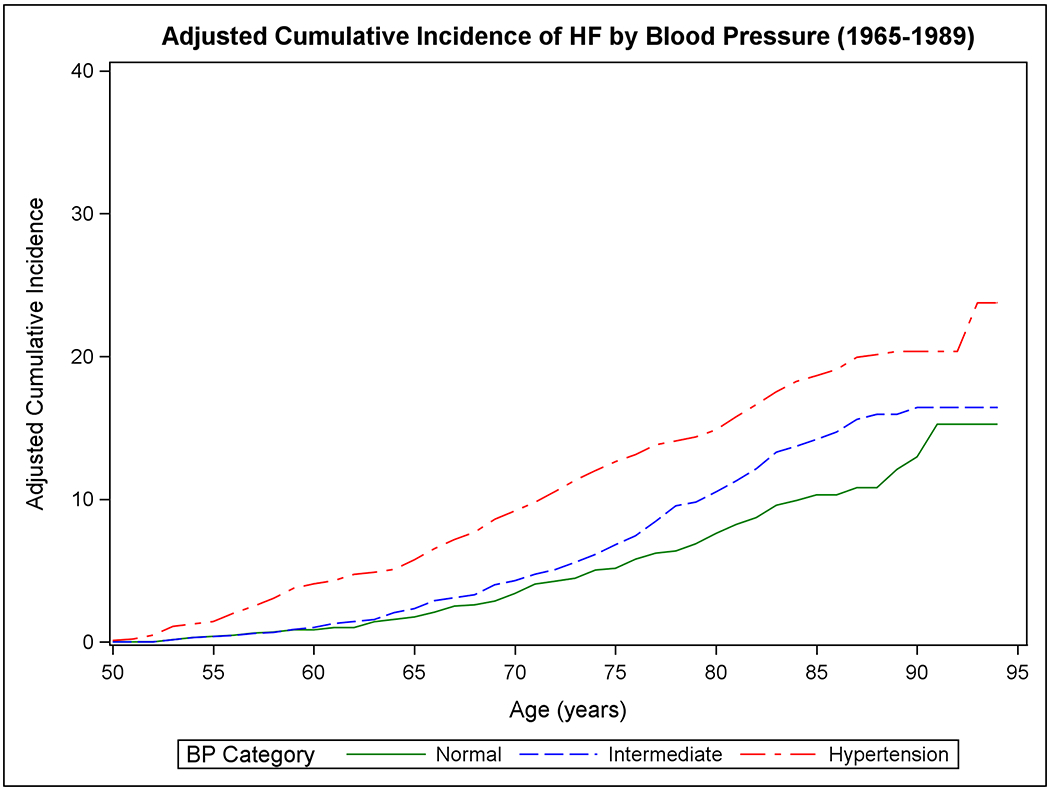
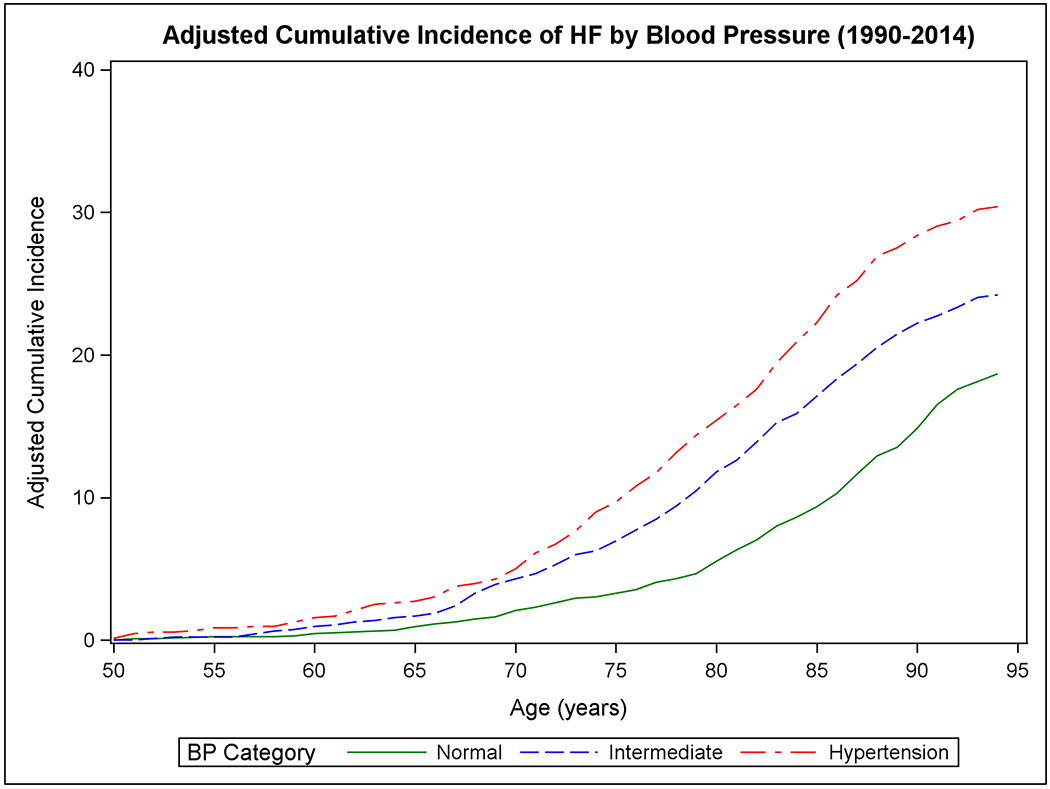
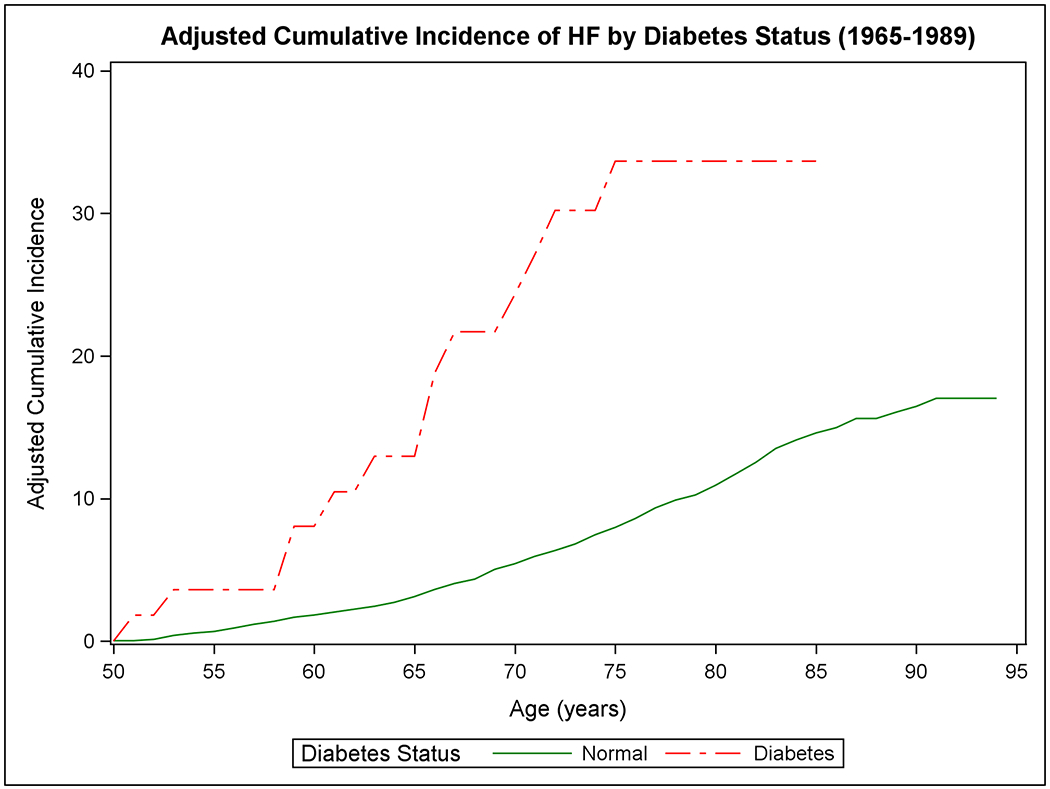
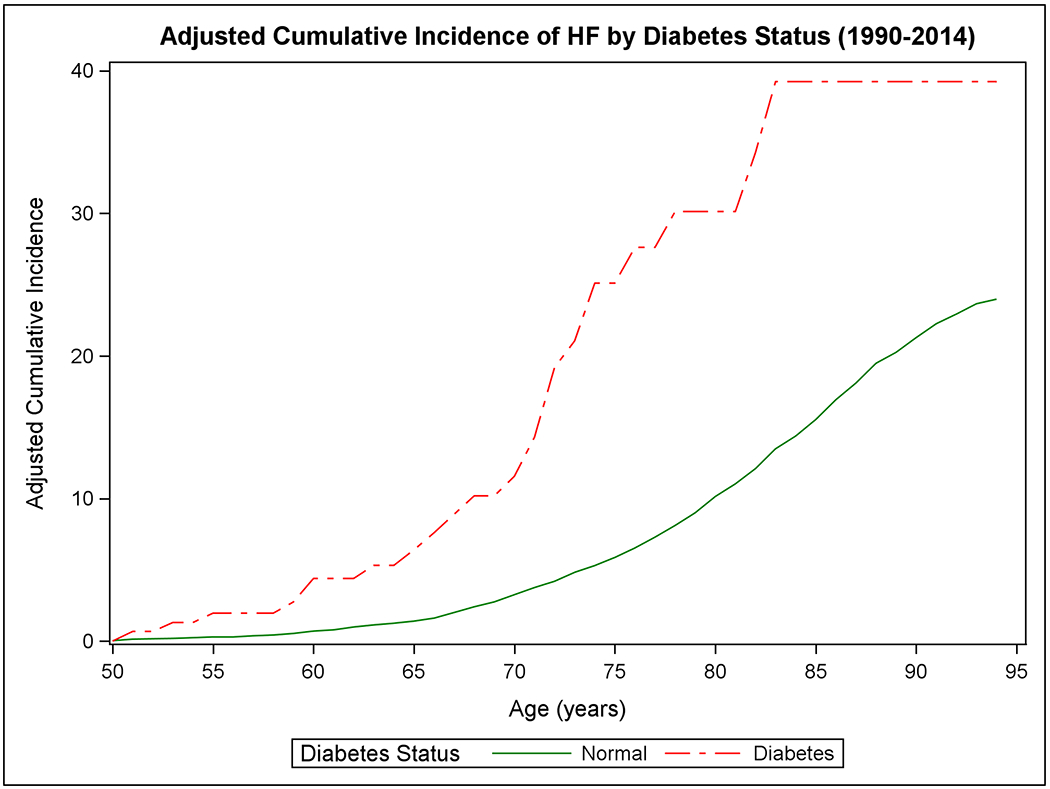
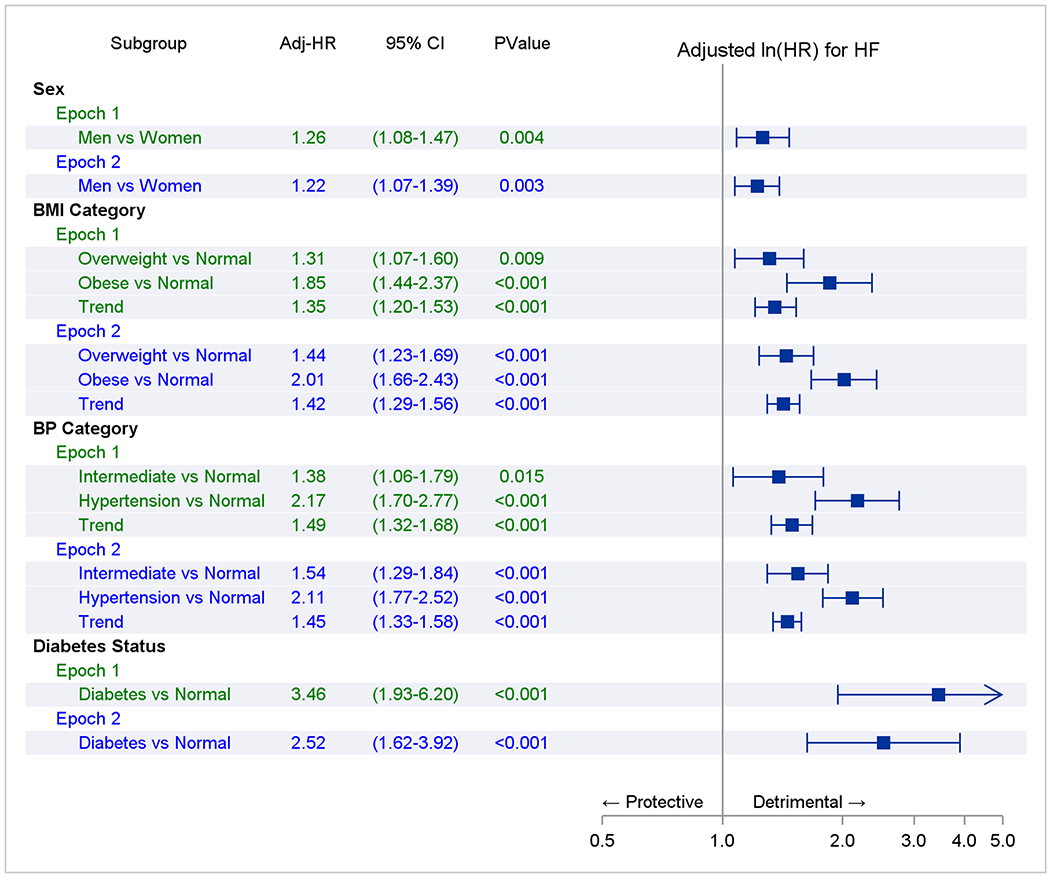
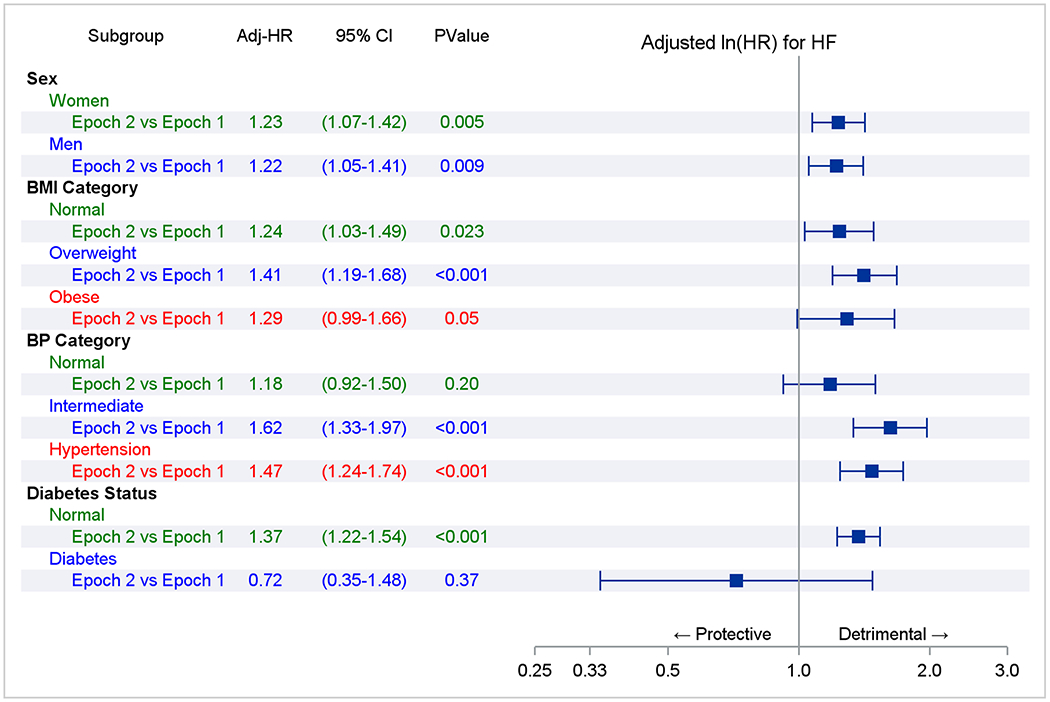
Methods: We compared the RLR of HF at age 50 years (adjusting for competing risk of death) in the 2 epochs in Framingham Study participants overall and in the following strata: sex, body mass index, blood pressure, and diabetes.
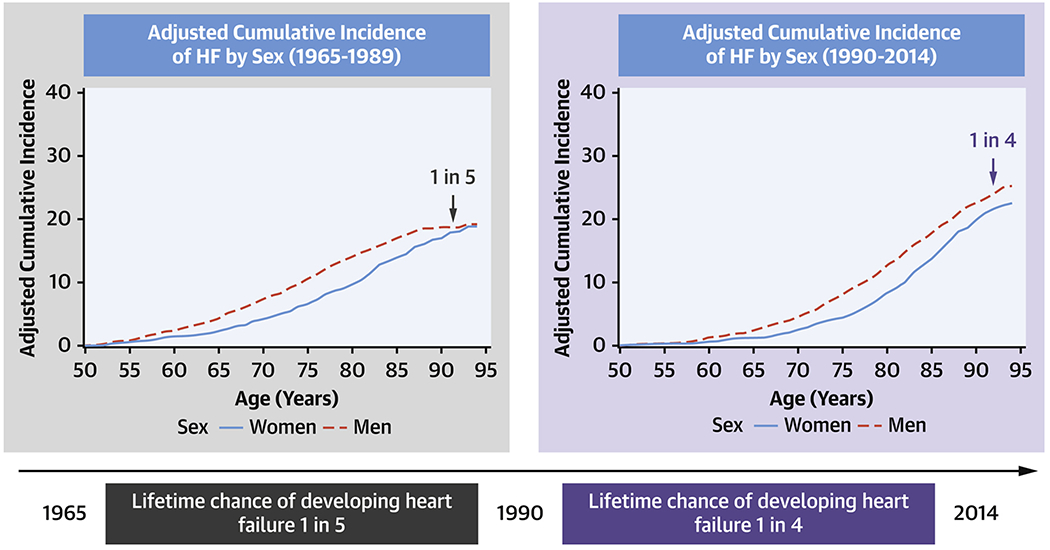
Results: Mean life expectancy increased from 75.9 to 82.1 years in women and 72.5 to 78.1 years in men. We observed 624 HF events over 111,351 person-observations in epoch 1, and 875 HF events over 128,903 person-observations in epoch 2. The mean age at onset of HF increased across the epochs by 6.6 years (women) to 7.2 years (men). The RLR of HF at age 50 years increased across epochs from 18.86% to 22.55% (absolute increase 3.69; 95% CI: 0.90-6.49; P = 0.01) in women, and from 19.19% to 25.25% (absolute increase 6.06; 95% CI: 3.08-9.04; P < 0.001) in men. The increase in RLR of HF in the second epoch was consistent across strata with excess body mass index or higher blood pressure (relative increase of 28%-47%) and in participants without prior myocardial infarction (relative increase of 23%).
Conclusions: The RLR of HF has increased in our community-based sample of White individuals over the last 5 decades, possibly caused by an increase in life expectancy.
Keywords: cohort studies; epidemiology; heart failure; lifetime risk; period effects.
Copyright © 2022 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This work is supported by Contracts NO1-HC-25195, HHSN268201500001I, and 75N92019D00031 from the National Heart, Lung, and Blood Institute. Dr Vasan is supported in part by the Evans Medical Foundation and the Jay and Louis Coffman Endowment from the Department of Medicine, Boston University School of Medicine. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Change in Lifetime Risk of Heart Failure: Applicable to All?J Am Coll Cardiol. 2022 Jan 25;79(3):264-266. doi: 10.1016/j.jacc.2021.11.014. J Am Coll Cardiol. 2022. PMID: 35057912 No abstract available.
References
-
- Virani SS, Alonso A, Aparicio HJ et al. Heart Disease and Stroke Statistics;2021 Update. Circulation 2021;143:e254–e743. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
