

Vectorized Treg-depleting αCTLA-4 elicits antigen cross-presentation and CD8+ T cell immunity to reject 'cold' tumors
- PMID: 35058324
- PMCID: PMC8783833
- DOI: 10.1136/jitc-2021-003488
Vectorized Treg-depleting αCTLA-4 elicits antigen cross-presentation and CD8+ T cell immunity to reject 'cold' tumors
Abstract
Background: Immune checkpoint blockade (ICB) is a clinically proven concept to treat cancer. Still, a majority of patients with cancer including those with poorly immune infiltrated 'cold' tumors are resistant to currently available ICB therapies. Cytotoxic T lymphocyte-associated antigen-4 (CTLA-4) is one of few clinically validated targets for ICB, but toxicities linked to efficacy in approved αCTLA-4 regimens have restricted their use and precluded full therapeutic dosing. At a mechanistic level, accumulating preclinical and clinical data indicate dual mechanisms for αCTLA-4; ICB and regulatory T cell (Treg) depletion are both thought to contribute efficacy and toxicity in available, systemic, αCTLA-4 regimens. Accordingly, strategies to deliver highly effective, yet safe αCTLA-4 therapies have been lacking. Here we assess and identify spatially restricted exposure to a novel strongly Treg-depleting, checkpoint-blocking, vectorized αCTLA-4, as a highly efficacious and potentially safe strategy to target CTLA-4.
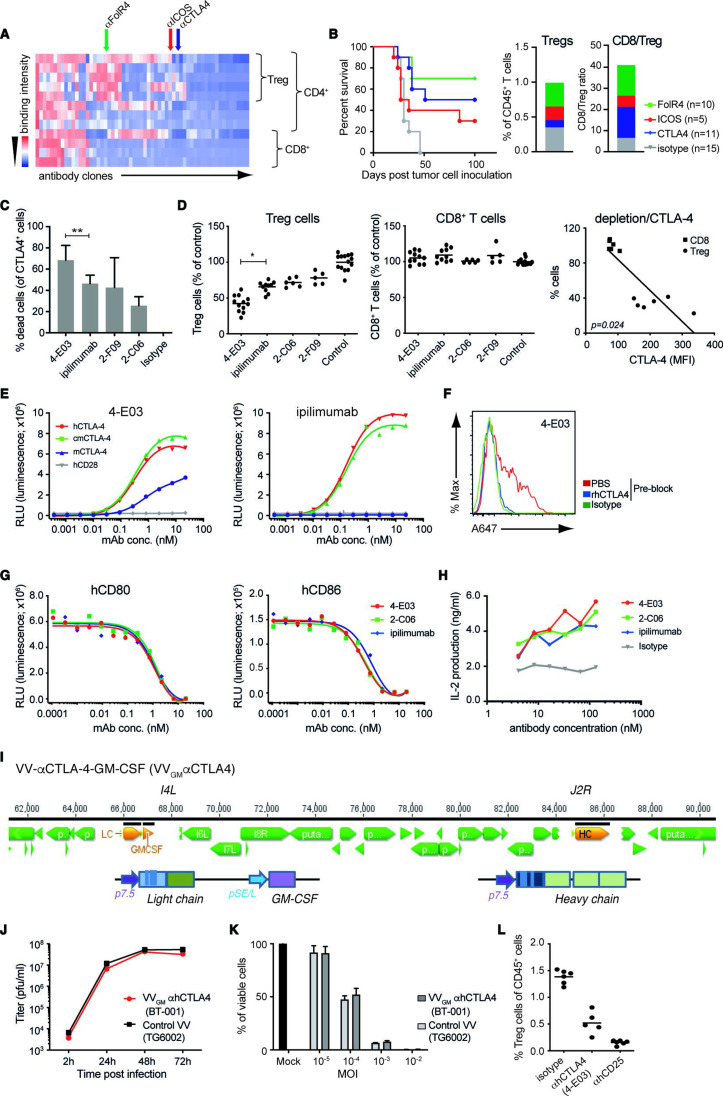
Methods: A novel human IgG1 CTLA-4 antibody (4-E03) was identified using function-first screening for monoclonal antibodies (mAbs) and targets associated with superior Treg-depleting activity. A tumor-selective oncolytic vaccinia vector was then engineered to encode this novel, strongly Treg-depleting, checkpoint-blocking, αCTLA-4 antibody or a matching surrogate antibody, and Granulocyte-macrophage colony-stimulating factor (GM-CSF) (VVGM-αCTLA-4).
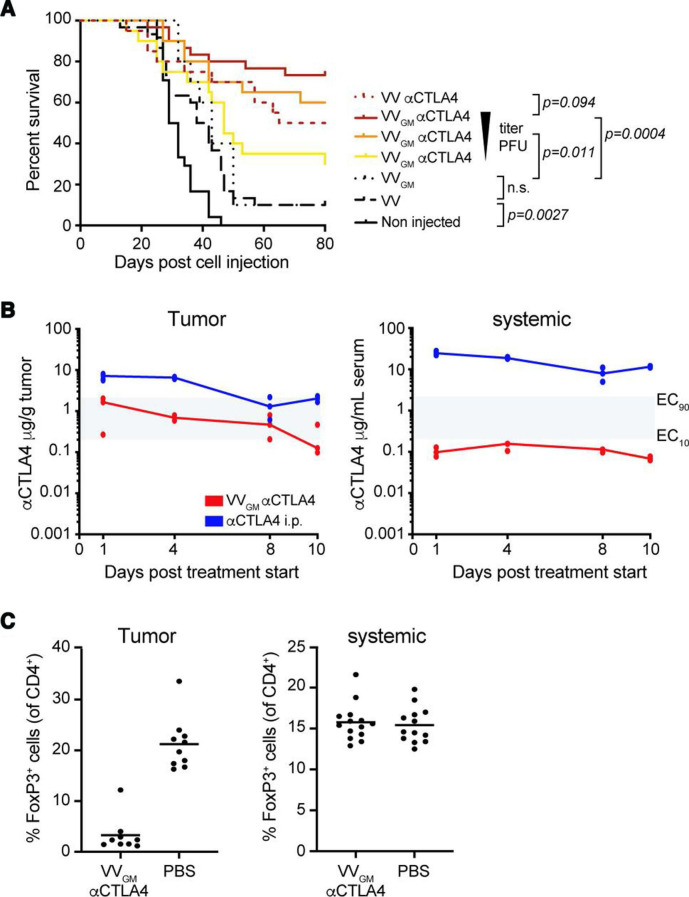
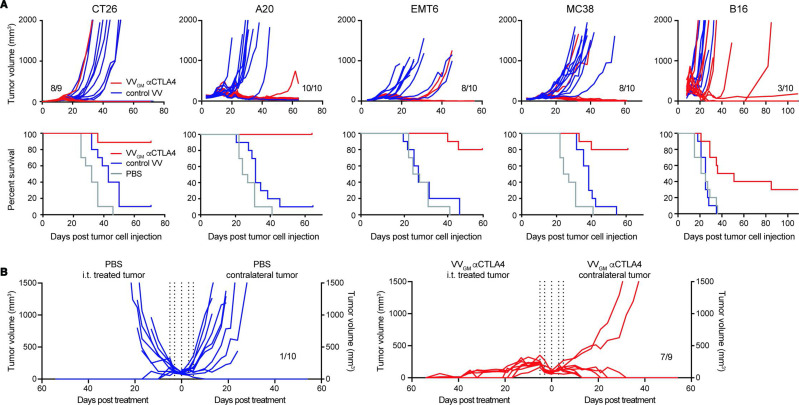
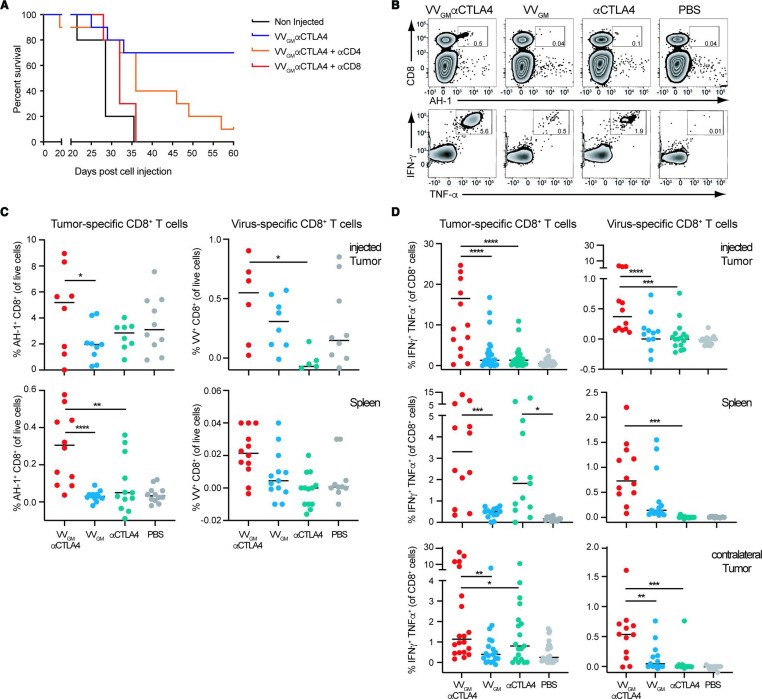
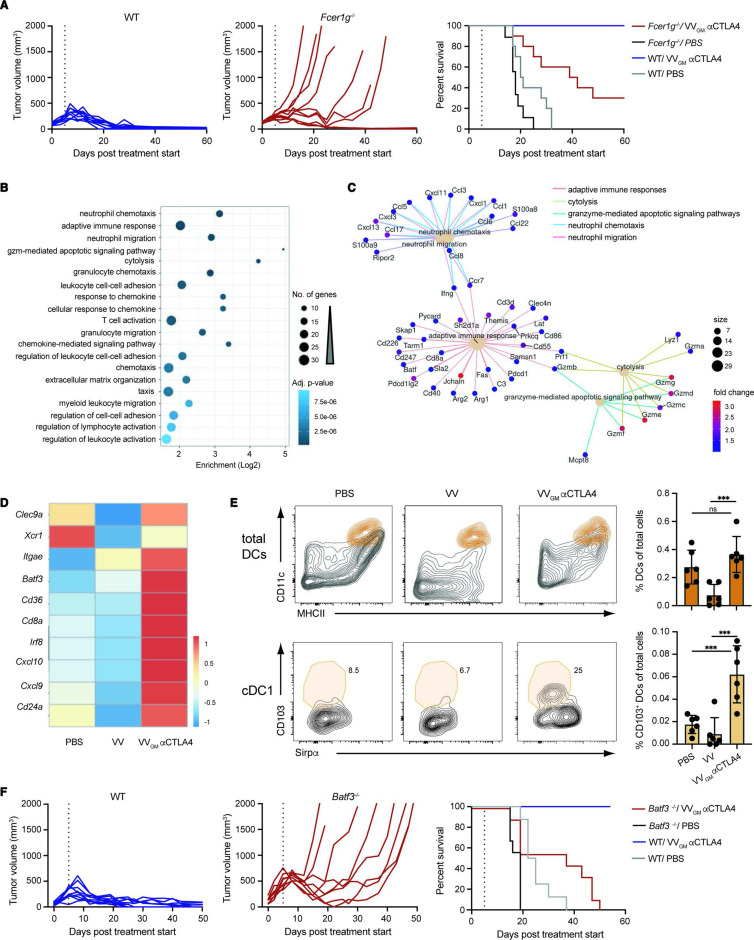
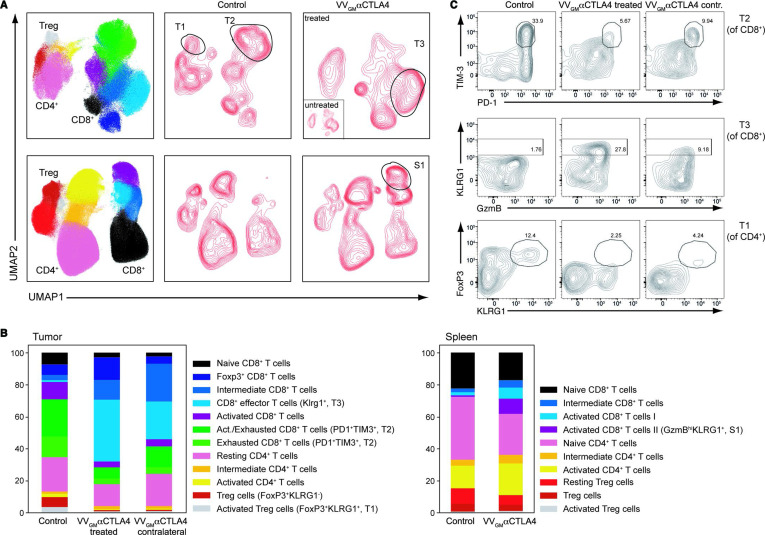
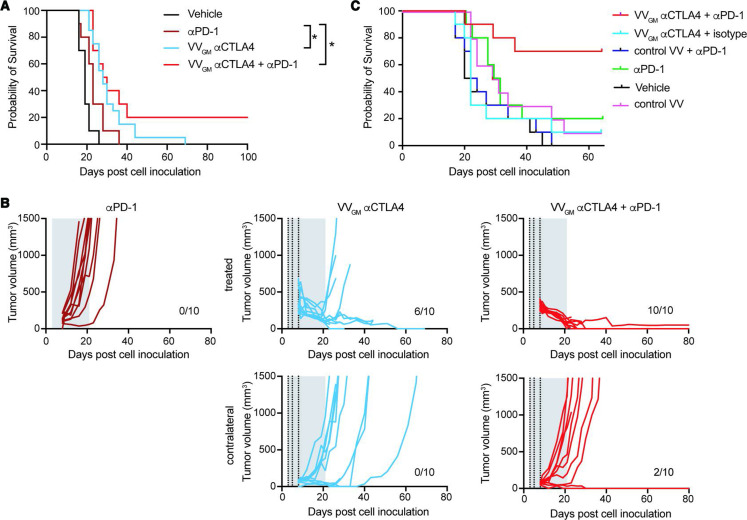
Results: The identified 4-E03 antibody showed significantly stronger Treg depletion, but equipotent checkpoint blockade, compared with clinically validated αCTLA-4 ipilimumab against CTLA-4-expressing Treg cells in a humanized mouse model in vivo. Intratumoral administration of VVGM-αCTLA-4 achieved tumor-restricted CTLA-4 receptor saturation and Treg depletion, which elicited antigen cross-presentation and stronger systemic expansion of tumor-specific CD8+ T cells and antitumor immunity compared with systemic αCTLA-4 antibody therapy. Efficacy correlated with FcγR-mediated intratumoral Treg depletion. Remarkably, in a clinically relevant mouse model resistant to systemic ICB, intratumoral VVGM-αCTLA-4 synergized with αPD-1 to reject cold tumors.
Conclusion: Our findings demonstrate in vivo proof of concept for spatial restriction of Treg depletion-optimized immune checkpoint blocking, vectorized αCTLA-4 as a highly effective and safe strategy to target CTLA-4. A clinical trial evaluating intratumoral VVGM-αhCTLA-4 (BT-001) alone and in combination with αPD-1 in metastatic or advanced solid tumors has commenced.
Keywords: CTLA-4 antigen; antibody specificity; immunotherapy; oncolytic virotherapy.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: MS, MR, PH, LM, CS, FJ, MB, IT, and BF are employees, MS, MR, LM, FJ, MB, IT, and BF are shareholders of BioInvent International. KLC received funding from BioInvent. J-BM, LF, CR, NS, PK, JD, JF, and EQ are employees and shareholders of Transgene.
Figures
Similar articles
-
Oncolytic virus expressing PD-1 inhibitors activates a collaborative intratumoral immune response to control tumor and synergizes with CTLA-4 or TIM-3 blockade.J Immunother Cancer. 2022 Jun;10(6):e004762. doi: 10.1136/jitc-2022-004762. J Immunother Cancer. 2022. PMID: 35688558 Free PMC article.
-
Combination of tumor site-located CTL-associated antigen-4 blockade and systemic regulatory T-cell depletion induces tumor-destructive immune responses.Cancer Res. 2007 Jun 15;67(12):5929-39. doi: 10.1158/0008-5472.CAN-06-4296. Cancer Res. 2007. PMID: 17575163
-
Cytotoxic T lymphocyte-associated protein 4 antibody aggrandizes antitumor immune response of oncolytic virus M1 via targeting regulatory T cells.Int J Cancer. 2021 Sep 15;149(6):1369-1384. doi: 10.1002/ijc.33703. Epub 2021 Jun 11. Int J Cancer. 2021. PMID: 34086978
-
Preserving the CTLA-4 Checkpoint for Safer and More Effective Cancer Immunotherapy.Trends Pharmacol Sci. 2020 Jan;41(1):4-12. doi: 10.1016/j.tips.2019.11.003. Epub 2019 Dec 10. Trends Pharmacol Sci. 2020. PMID: 31836191 Free PMC article. Review.
-
Targeting immune checkpoints in hematological malignancies.J Hematol Oncol. 2020 Aug 12;13(1):111. doi: 10.1186/s13045-020-00947-6. J Hematol Oncol. 2020. PMID: 32787882 Free PMC article. Review.
Cited by
-
Current clinical landscape of oncolytic viruses as novel cancer immunotherapeutic and recent preclinical advancements.Front Immunol. 2022 Aug 25;13:953410. doi: 10.3389/fimmu.2022.953410. eCollection 2022. Front Immunol. 2022. PMID: 36091031 Free PMC article. Review.
-
Foxp3 inhibitory peptide encapsulated in a novel CD25-targeted nanoliposome promotes efficient tumor regression in mice.Acta Pharmacol Sin. 2025 Jan;46(1):171-183. doi: 10.1038/s41401-024-01338-0. Epub 2024 Jul 29. Acta Pharmacol Sin. 2025. PMID: 39075226 Free PMC article.
-
Sequence enrichment profiles enable target-agnostic antibody generation for a broad range of antigens.Cell Rep Methods. 2023 May 9;3(5):100475. doi: 10.1016/j.crmeth.2023.100475. eCollection 2023 May 22. Cell Rep Methods. 2023. PMID: 37323567 Free PMC article.
-
Harnessing the tumor microenvironment to boost adoptive T cell therapy with engineered lymphocytes for solid tumors.Semin Immunopathol. 2024 Jul 25;46(3-4):8. doi: 10.1007/s00281-024-01011-y. Semin Immunopathol. 2024. PMID: 39060547 Review.
-
Oncolytic vaccinia virus and cancer immunotherapy.Front Immunol. 2024 Jan 12;14:1324744. doi: 10.3389/fimmu.2023.1324744. eCollection 2023. Front Immunol. 2024. PMID: 38283361 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials