

Finerenone in Patients With Chronic Kidney Disease and Type 2 Diabetes According to Baseline HbA1c and Insulin Use: An Analysis From the FIDELIO-DKD Study
- PMID: 35061867
- PMCID: PMC9271031
- DOI: 10.2337/dc21-1944
Finerenone in Patients With Chronic Kidney Disease and Type 2 Diabetes According to Baseline HbA1c and Insulin Use: An Analysis From the FIDELIO-DKD Study
Erratum in
-
Erratum. Finerenone in Patients With Chronic Kidney Disease and Type 2 Diabetes According to Baseline HbA1c and Insulin Use: An Analysis From the FIDELIO-DKD Study. Diabetes Care 2022;45:888-897.Diabetes Care. 2023 Sep 1;46(9):1721. doi: 10.2337/dc23-er09. Diabetes Care. 2023. PMID: 37310695 Free PMC article. No abstract available.
Abstract
Objective: Finerenone significantly improved cardiorenal outcomes in patients with chronic kidney disease (CKD) and type 2 diabetes (T2D) in the Finerenone in Reducing Kidney Failure and Disease Progression in Diabetic Kidney Disease trial. We explored whether baseline HbA1c level and insulin treatment influenced outcomes.
Research design and methods: Patients with T2D, urine albumin-to-creatinine ratio (UACR) of 30-5,000 mg/g, estimated glomerular filtration rate (eGFR) of 25 to <75 mL/min/1.73 m2, and treated with optimized renin-angiotensin system blockade were randomly assigned to receive finerenone or placebo. Efficacy outcomes included kidney (kidney failure, sustained decrease ≥40% in eGFR from baseline, or renal death) and cardiovascular (cardiovascular death, nonfatal myocardial infarction, nonfatal stroke, or hospitalization for heart failure) composite endpoints. Patients were analyzed by baseline insulin use and by baseline HbA1c <7.5% (58 mmol/mol) or ≥7.5%.
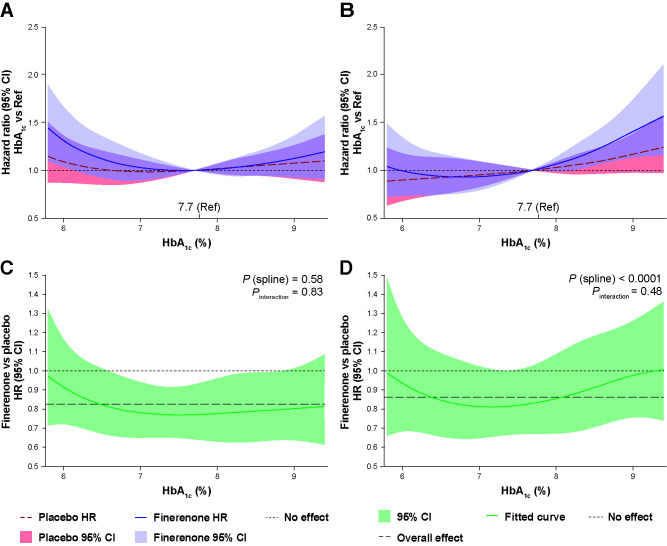
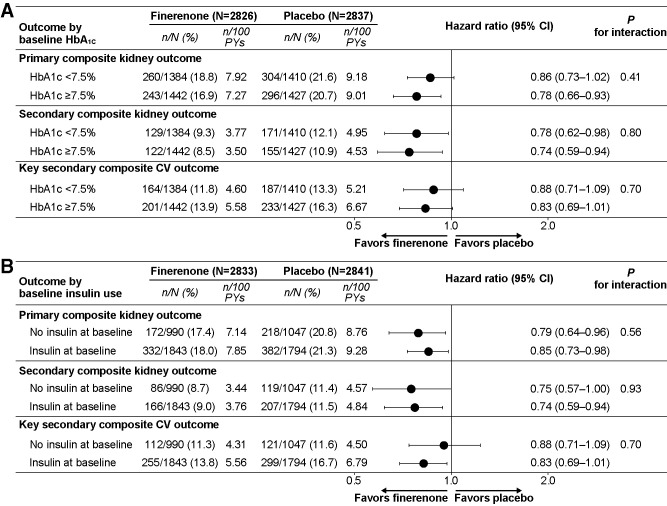
Results: Of 5,674 patients, 3,637 (64.1%) received insulin at baseline. Overall, 5,663 patients were included in the analysis for HbA1c; 2,794 (49.3%) had baseline HbA1c <7.5% (58 mmol/mol). Finerenone significantly reduced risk of the kidney composite outcome independent of baseline HbA1c level and insulin use (Pinteraction = 0.41 and 0.56, respectively). Cardiovascular composite outcome incidence was reduced with finerenone irrespective of baseline HbA1c level and insulin use (Pinteraction = 0.70 and 0.33, respectively). Although baseline HbA1c level did not affect kidney event risk, cardiovascular risk increased with higher HbA1c level. UACR reduction was consistent across subgroups. Adverse events were similar between groups regardless of baseline HbA1c level and insulin use; few finerenone-treated patients discontinued treatment because of hyperkalemia.
Conclusions: Finerenone reduces kidney and cardiovascular outcome risk in patients with CKD and T2D, and risks appear consistent irrespective of HbA1c levels or insulin use.
Trial registration: ClinicalTrials.gov NCT02540993.
© 2022 by the American Diabetes Association.
Figures
References
-
- International Diabetes Federation . IDF Diabetes Atlas. 9th ed. Brussels, Belgium, International Diabetes Federation, 2019
-
- Kidney Disease: Improving Global Outcomes (KDIGO) Diabetes Work Group . KDIGO 2020 clinical practice guideline for diabetes management in chronic kidney disease. Kidney Int 2020;98:S1–S115 - PubMed
-
- American Diabetes Association . 6. Glycemic targets: standards of medical care in diabetes–2021. Diabetes Care 2021;44(Suppl. 1):S73–S84 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
