

Wearable Sensors and Machine Learning for Hypovolemia Problems in Occupational, Military and Sports Medicine: Physiological Basis, Hardware and Algorithms
- PMID: 35062401
- PMCID: PMC8781307
- DOI: 10.3390/s22020442
Wearable Sensors and Machine Learning for Hypovolemia Problems in Occupational, Military and Sports Medicine: Physiological Basis, Hardware and Algorithms
Abstract
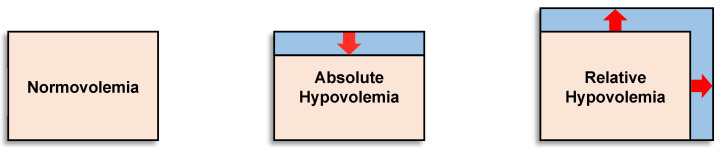
Hypovolemia is a physiological state of reduced blood volume that can exist as either (1) absolute hypovolemia because of a lower circulating blood (plasma) volume for a given vascular space (dehydration, hemorrhage) or (2) relative hypovolemia resulting from an expanded vascular space (vasodilation) for a given circulating blood volume (e.g., heat stress, hypoxia, sepsis). This paper examines the physiology of hypovolemia and its association with health and performance problems common to occupational, military and sports medicine. We discuss the maturation of individual-specific compensatory reserve or decompensation measures for future wearable sensor systems to effectively manage these hypovolemia problems. The paper then presents areas of future work to allow such technologies to translate from lab settings to use as decision aids for managing hypovolemia. We envision a future that incorporates elements of the compensatory reserve measure with advances in sensing technology and multiple modalities of cardiovascular sensing, additional contextual measures, and advanced noise reduction algorithms into a fully wearable system, creating a robust and physiologically sound approach to manage physical work, fatigue, safety and health issues associated with hypovolemia for workers, warfighters and athletes in austere conditions.
Keywords: cardiac decompensation; compensatory reserve; dehydration; environmental stress and adaptation; physical work capabilities; wearable sensors.
Conflict of interest statement
O.T.I. is a Scientific Advisor to Physiowave, Inc. and a Co-Founder, Chief Scientific Advisor, and Board Member for Cardiosense, Inc. The other authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
Similar articles
-
Wearable technology for compensatory reserve to sense hypovolemia.J Appl Physiol (1985). 2018 Feb 1;124(2):442-451. doi: 10.1152/japplphysiol.00264.2017. Epub 2017 Jul 27. J Appl Physiol (1985). 2018. PMID: 28751369 Review.
-
Classification of Blood Volume Decompensation State via Machine Learning Analysis of Multi-Modal Wearable-Compatible Physiological Signals.Sensors (Basel). 2022 Feb 10;22(4):1336. doi: 10.3390/s22041336. Sensors (Basel). 2022. PMID: 35214238 Free PMC article.
-
Wearable Sensors Incorporating Compensatory Reserve Measurement for Advancing Physiological Monitoring in Critically Injured Trauma Patients.Sensors (Basel). 2020 Nov 10;20(22):6413. doi: 10.3390/s20226413. Sensors (Basel). 2020. PMID: 33182638 Free PMC article. Review.
-
AI-Enabled Advanced Development for Assessing Low Circulating Blood Volume for Emergency Medical Care: Comparison of Compensatory Reserve Machine-Learning Algorithms.Sensors (Basel). 2022 Mar 30;22(7):2642. doi: 10.3390/s22072642. Sensors (Basel). 2022. PMID: 35408255 Free PMC article.
-
Unifying the Estimation of Blood Volume Decompensation Status in a Porcine Model of Relative and Absolute Hypovolemia Via Wearable Sensing.IEEE J Biomed Health Inform. 2021 Sep;25(9):3351-3360. doi: 10.1109/JBHI.2021.3068619. Epub 2021 Sep 3. IEEE J Biomed Health Inform. 2021. PMID: 33760744
Cited by
-
Artificial Intelligence and Occupational Health and Safety, Benefits and Drawbacks.Med Lav. 2024 Apr 24;115(2):e2024014. doi: 10.23749/mdl.v115i2.15835. Med Lav. 2024. PMID: 38686574 Free PMC article.
-
A Comparison of Normalization Techniques for Individual Baseline-Free Estimation of Absolute Hypovolemic Status Using a Porcine Model.Biosensors (Basel). 2024 Jan 23;14(2):61. doi: 10.3390/bios14020061. Biosensors (Basel). 2024. PMID: 38391980 Free PMC article.
References
-
- Castellani J.W., Muza S.R., Cheuvront S.N., Sils I.V., Fulco C.S., Kenefick R.W., Beidleman B.A., Sawka M.N. Effect of hypohydration and altitude exposure on aerobic exercise performance and acute mountain sickness. J. Appl. Physiol. 2010;109:1792–1800. doi: 10.1152/japplphysiol.00517.2010. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
