

Transition to invasive breast cancer is associated with progressive changes in the structure and composition of tumor stroma
- PMID: 35063072
- PMCID: PMC8792442
- DOI: 10.1016/j.cell.2021.12.023
Transition to invasive breast cancer is associated with progressive changes in the structure and composition of tumor stroma
Abstract
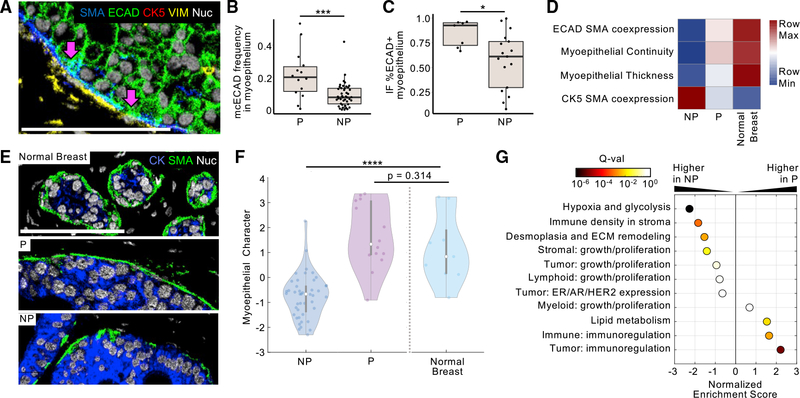
Ductal carcinoma in situ (DCIS) is a pre-invasive lesion that is thought to be a precursor to invasive breast cancer (IBC). To understand the changes in the tumor microenvironment (TME) accompanying transition to IBC, we used multiplexed ion beam imaging by time of flight (MIBI-TOF) and a 37-plex antibody staining panel to interrogate 79 clinically annotated surgical resections using machine learning tools for cell segmentation, pixel-based clustering, and object morphometrics. Comparison of normal breast with patient-matched DCIS and IBC revealed coordinated transitions between four TME states that were delineated based on the location and function of myoepithelium, fibroblasts, and immune cells. Surprisingly, myoepithelial disruption was more advanced in DCIS patients that did not develop IBC, suggesting this process could be protective against recurrence. Taken together, this HTAN Breast PreCancer Atlas study offers insight into drivers of IBC relapse and emphasizes the importance of the TME in regulating these processes.
Keywords: DCIS; MIBI; breast cancer; myoepithelium; spatial proteomics; systems biology; tumor microenvironment; tumor progression.
Copyright © 2022 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests M.A. and S.C.B. are inventors on patent US20150287578A1. M.A. and S.C.B. are board members and shareholders in IonPath Inc. T.R. and E.F.M. have previously consulted for IonPath Inc.
Figures





References
-
- Aguiar FN, Cirqueira CS, Bacchi CE, and Carvalho FM (2015). Morphologic, molecular and microenvironment factors associated with stromal invasion in breast ductal carcinoma in situ: Role of myoepithelial cells. Breast Dis. 35, 249–252. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
