

Safety and antitumor activity of dostarlimab in patients with advanced or recurrent DNA mismatch repair deficient/microsatellite instability-high (dMMR/MSI-H) or proficient/stable (MMRp/MSS) endometrial cancer: interim results from GARNET-a phase I, single-arm study
- PMID: 35064011
- PMCID: PMC8785197
- DOI: 10.1136/jitc-2021-003777
Safety and antitumor activity of dostarlimab in patients with advanced or recurrent DNA mismatch repair deficient/microsatellite instability-high (dMMR/MSI-H) or proficient/stable (MMRp/MSS) endometrial cancer: interim results from GARNET-a phase I, single-arm study
Abstract
Background: Dostarlimab is a humanized monoclonal antibody that binds with high affinity to PD-1, resulting in inhibition of binding to PD-L1 and PD-L2. We report interim data from patients with endometrial cancer (EC) participating in a phase I trial of single-agent dostarlimab.
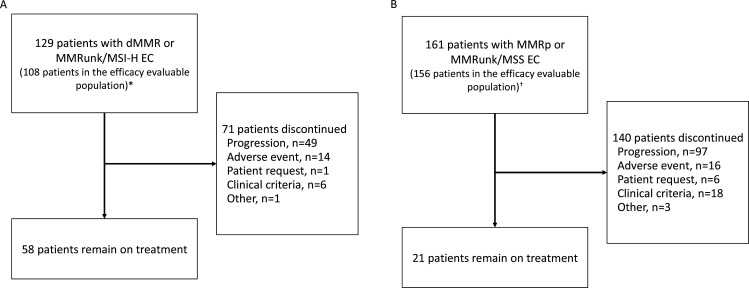
Methods: GARNET, an ongoing, single-arm, open-label, phase I trial of intravenous dostarlimab in advanced solid tumors, is being undertaken at 123 sites. Two cohorts of patients with EC were recruited: those with dMMR/MSI-H disease (cohort A1) and those with proficient/stable (MMRp/MSS) disease (cohort A2). Patients received dostarlimab 500 mg every 3 weeks for 4 cycles, then dostarlimab 1000 mg every 6 weeks until disease progression. The primary endpoints were objective response rate (ORR) and duration of response (DOR) per RECIST V.1.1, as assessed by blinded independent central review.
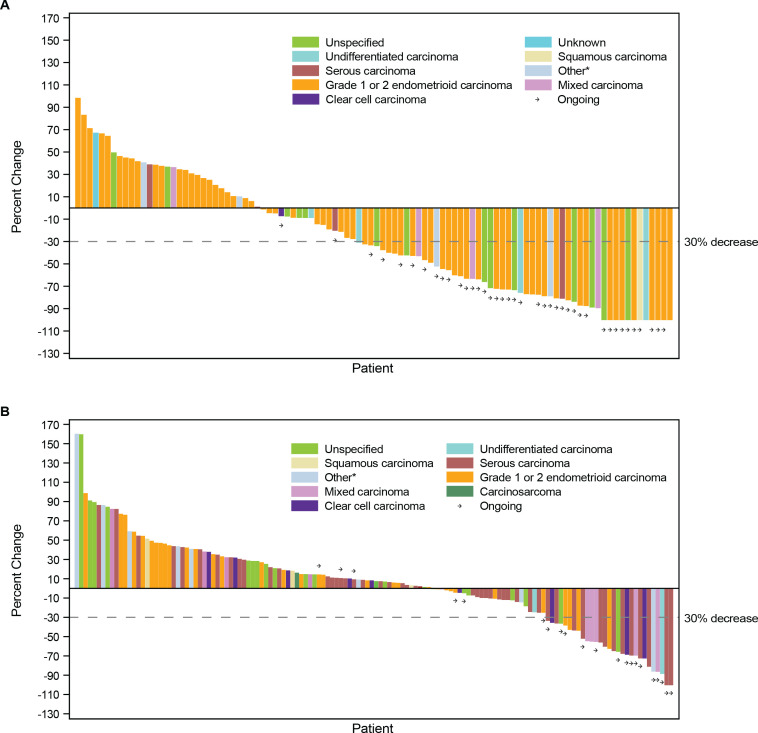
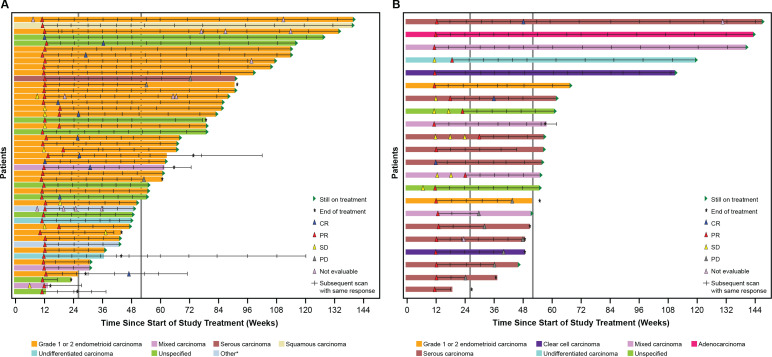
Results: Screening began on April 10, 2017, and 129 and 161 patients with advanced EC were enrolled in cohorts A1 and A2, respectively. The median follow-up duration was 16.3 months (IQR 9.5-22.1) for cohort A1 and 11.5 months (IQR 11.0-25.1) for cohort A2. In cohort A1, ORR was 43.5% (95% CI 34.0% to 53.4%) with 11 complete responses and 36 partial responses. In cohort A2, ORR was 14.1% (95% CI 9.1% to 20.6%) with three complete responses and 19 partial responses. Median DOR was not reached in either cohort. In the combined cohorts, the majority of treatment-related adverse events (TRAEs) were grade 1-2 (75.5%), most commonly fatigue (17.6%), diarrhea (13.8%), and nausea (13.8%). Grade≥3 TRAEs occurred in 16.6% of patients, and 5.5% discontinued dostarlimab because of TRAEs. No deaths were attributable to dostarlimab.
Conclusion: Dostarlimab demonstrated durable antitumor activity in both dMMR/MSI-H (ORR 43.5%) and MMRp/MSS EC (ORR 14.1%) with a manageable safety profile.
Trial registration number: NCT02715284.
Keywords: clinical trials as topic; immunotherapy; programmed cell death 1 receptor.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: AO reports consulting fees from AstraZeneca, Bristol Meyers Squibb, Deciphera Pharmaceutical, Genmab, GlaxoSmithKline, ImmunoGen, Mersana Therapeutics, SUTRA, and Roche; institutional grants from Abbie Deutschland, Ability Pharmaceuticals, Advaxis Inc, Aeterna Zentaris, Amgen SA, Aprea Therapeutics AB, Clovis Oncology Inc, Eisai Ltd, F. Hoffmann-La Roche Ltd, GlaxoSmithKline, ImmunoGen Inc, and Merck Sharp & Dohme de Espana SA, Millennium Pharmaceuticals Inc, PharmaMar, and Regeneron Pharmaceuticals, and travel support from AstraZeneca, Clovis Oncology, PharmaMar, and Roche. LG reports institutional grants from AstraZeneca, Pfizer, and Merck Sharp & Dohme, Karyopharm, Tesaro, IMV, Alkermes, Clovis, ImmunoGen Inc, Roche, Mersana, Esperas, Novocure GmbH, OncoQuest Pharmaceuticals; consulting fees from Merck; honoraria from AstraZeneca, GlaxoSmithKline, Eisai, Eisai-Merck, and Alkermes. AVT reports institutional grants from AstraZeneca and personal fees from AstraZeneca and Eisai. JB reports honoraria from Olympus; consulting or advisory role at Caris, GlaxoSmithKline, Clovis, AstraZeneca, and Genentech; and speakers’ bureau at Clovis. CM reports institutional grants from GlaxoSmithKline. JP has nothing to disclose. RS reports institutional grants from AstraZeneca and Eisai; personal fees from AstraZeneca, GlaxoSmithKline, Novartis, Pfizer, and Roche; and nonfinancial support from Amgen, AstraZeneca, Pfizer, and Roche. DMO'M reports personal fees from Agenus, Array Biopharma, Eisai, GlaxoSmithKline, and ImmunoGen; consultant/advisory board for Abbvie, Ambry, Amgen, Clovis, EMD Serono, Ergomed, Janssen/J&J, Myriad Genetics, Novacure, Regeneron, Tarveda, and VentiRx; steering committee for Genentech/Roche and Merck; institutional funding from Ajinomoto Inc, Bristol Myers Squibb, Cerulean Pharma, GOG Foundation, INC Research Inc, Inventiv Health Clinical, Iovance Biotherapeutics Inc, Ludwig Cancer Research, New Mexico Cancer Care Alliance, PRA International, Serono Inc, Stemcentrx Inc, Tracon Pharmaceuticals, and Yale University. VS has nothing to disclose. VB reports consulting or advisory roles at Guidepoint Global and OncoArt; speakers’ bureau fees from Solti; travel support from START; honoraria from Loxo and IDEAYA Biosciences; and institutional grants from Abbvie, Adaptimmune, Alkermes, Amgen, Array BioPharma, AstraZeneca, Bayer, BioNTech AG, Boehringer Ingelheim, Boston Biomedical, Bristol Myers Squibb, CytomX Therapeutics, Genmab, GlaxoSmithKline, Incyte, Janssen Oncology, Kura Oncology, Lilly, Loxo, Menarini, Merck, Merus, Novartis, Pfizer, Pumo Biotechnology, Roche/Genentech, Sanofi, Seattle Genetics, Synthon, and Zenith Epigenetics. LD reports personal fees from Advance Medical, ASCO, AstraZeneca, British Journal of OB/GYN, ClearView Health Care, Cue Biopharma, Elsevier, Genentech/Roche, Innovio, JB Learning, Merck, MorphoTek, National Cancer Institute, Parexel, State of California, and UpToDate; and institutional grants from Abbvie, Advaxis, Aduro BioTech, Cerulean/NextGen, Eisai, Genentech/Roche, GlaxoSmithKline, Inovio, LEAP Therapeutics, Ludwig, Lycera, Morab, Morphotek, Merck, Novartis, Pfizer, and Syndax. SG reports consulting or advisory role from Seattle Genetics; speakers’ bureau fees from GlaxoSmithKline; and institutional research funding from Abbvie, Advaxis, Bristol Myers Squibb, Clovis, Genentech, GlaxoSmithKline, Merck, Roche, Seattle Genetics, and Takeda. PG has nothing to disclose. RK reports personal fees from GlaxoSmithKline. CL reports contracted research for GlaxoSmithKline and scientific advisory board fees from GlaxoSmithKline, Eisai, Clovis Oncology, Seattle Genetics, and AbbVie. WG is a former employee of GlaxoSmithKline. EI is a former employee of GlaxoSmithKline. SZ, XH, TD, and JV are employees of GlaxoSmithKline. BP reports institutional grants support from Tesaro/GSK, AstraZeneca, Merck, Genentech/Roche, Celsion, Mersana, Karyopharm, and Clovis Oncology; and advisory board fees from Tesaro/GSK, AstraZeneca, Merck, Eisai, Toray, Mersana, Elevar Therapeutics, Arquer Diagnostics, Sutro Biopharma, and Clovis Oncology.
Figures
References
-
- Upadhaya S, Yu A. FDA approval timeline of active immunotherapies: timeline of anti-PD-1/L1 antibody approvals by the FDA. Available: https://www.cancerresearch.org/en-us/scientists/immuno-oncology-landscap... [Accessed 21 Aug 2021].
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous