

Characteristics and outcome of facial nerve palsy from Lyme neuroborreliosis in the United States
- PMID: 35064770
- PMCID: PMC8791801
- DOI: 10.1002/acn3.51488
Characteristics and outcome of facial nerve palsy from Lyme neuroborreliosis in the United States
Abstract
Objectives: Facial palsy is the most common manifestation of Lyme neuroborreliosis (LNB) in the United States. This study aimed to describe features of patients with early LNB presenting with facial palsy and to determine if corticosteroids in addition to antibiotic therapy was associated with unfavorable outcome.
Methods: Retrospective analysis of participants enrolled in clinical studies investigating Lyme disease (N = 486) identified 44 patients who had facial palsy from LNB. The House-Brackmann scale was used to quantify the facial nerve dysfunction.
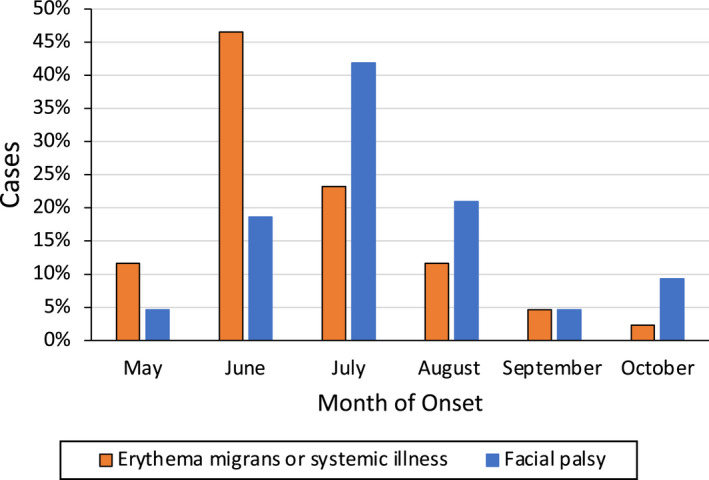
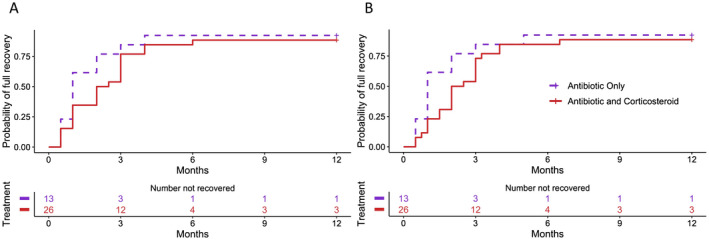
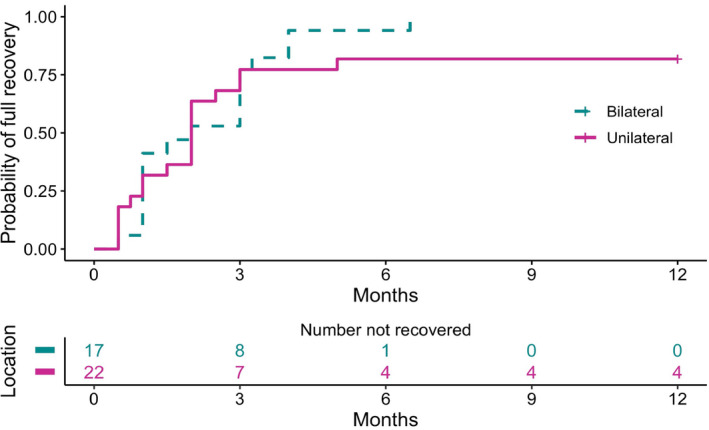
Results: Most patients presented in the summer months. Erythema migrans, frequently associated with systemic symptoms, occurred in 29 patients. Thirteen patients presented with bilateral facial palsy, usually with sequential involvement. Fourteen patients had painful radiculopathy. Of the 38 patients treated with antibiotics before the resolution of the palsy who had complete follow-up, 24 received both antibiotics and corticosteroids. Of these 38 patients, 34 recovered completely, 3 had nearly complete recovery, and 1 had moderate dysfunction. There were no differences between the treatment groups in achieving complete resolution of the palsy at 12 months or in time to complete recovery.
Interpretation: A history of rash compatible with erythema migrans or febrile illness in the weeks preceding the palsy are helpful clues pointing toward LNB and should be actively sought when evaluating patients with acute-onset peripheral facial palsy, particularly bilateral facial palsy. Treatment with antibiotic therapy is highly effective and most patients will fully recover facial nerve function. Adjunctive corticosteroid therapy appears to not affect the speed of recovery or overall outcome in this retrospective observational study.
Published 2022. This article is a U.S. Government work and is in the public domain in the USA. Annals of Clinical and Translational Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
AM has a patent US 8,926,989; and is an unpaid Scientific Advisor to the Global Lyme Alliance and to the American Lyme Disease Foundation. All other authors: no disclosures relevant to the manuscript.
Figures
Similar articles
-
Diagnosis and management of suspected Lyme neuroborreliosis-related facial nerve palsy in children by paediatricians and general practitioners: a French survey.Eur J Pediatr. 2024 Dec;183(12):5363-5370. doi: 10.1007/s00431-024-05780-4. Epub 2024 Oct 10. Eur J Pediatr. 2024. PMID: 39384650
-
Clinical characteristics of Lyme neuroborreliosis in Dutch children and adults.Eur J Pediatr. 2023 Mar;182(3):1183-1189. doi: 10.1007/s00431-022-04749-5. Epub 2023 Jan 6. Eur J Pediatr. 2023. PMID: 36607413
-
Clinical characteristics and cerebrospinal fluid parameters in patients with peripheral facial palsy caused by Lyme neuroborreliosis compared with facial palsy of unknown origin (Bell's palsy).BMC Infect Dis. 2011 Aug 10;11:215. doi: 10.1186/1471-2334-11-215. BMC Infect Dis. 2011. PMID: 21831262 Free PMC article.
-
Clinical manifestations of Lyme neuroborreliosis in children: a review.Eur J Pediatr. 2023 May;182(5):1965-1976. doi: 10.1007/s00431-023-04811-w. Epub 2023 Mar 1. Eur J Pediatr. 2023. PMID: 36856886 Review.
-
Efficacy and safety of pharmacological treatments for Lyme neuroborreliosis: An updated systematic review.Eur J Neurol. 2023 Dec;30(12):3780-3788. doi: 10.1111/ene.16034. Epub 2023 Sep 10. Eur J Neurol. 2023. PMID: 37565386
Cited by
-
Case Report: A Typical Lyme Disease With Uncommon Neurologic Presentation.J Community Hosp Intern Med Perspect. 2024 Sep 9;14(5):101-105. doi: 10.55729/2000-9666.1388. eCollection 2024. J Community Hosp Intern Med Perspect. 2024. PMID: 39399195 Free PMC article.
-
Persistent Symptoms After Treatment of Lyme Disease.Infect Dis Clin North Am. 2022 Sep;36(3):621-638. doi: 10.1016/j.idc.2022.04.004. Infect Dis Clin North Am. 2022. PMID: 36116839 Free PMC article. Review.
-
Lyme neuroborreliosis as a cause of sudden sensorineural hearing loss and facial palsy.Clin Case Rep. 2022 Oct 11;10(10):e6412. doi: 10.1002/ccr3.6412. eCollection 2022 Oct. Clin Case Rep. 2022. PMID: 36245466 Free PMC article.
-
Case presentation and management of Lyme disease patients: a 9-year retrospective analysis in France.Front Med (Lausanne). 2024 Jan 17;10:1296486. doi: 10.3389/fmed.2023.1296486. eCollection 2023. Front Med (Lausanne). 2024. PMID: 38298513 Free PMC article.
-
Unveiling Lyme Neuroborreliosis in the Absence of Dermatological Symptoms.Cureus. 2024 Dec 27;16(12):e76473. doi: 10.7759/cureus.76473. eCollection 2024 Dec. Cureus. 2024. PMID: 39867056 Free PMC article.
References
-
- Stanek G, Strle F. Lyme borreliosis‐from tick bite to diagnosis and treatment. FEMS Microbiol Rev. 2018;42(3):233‐258. - PubMed
-
- CDC . Lyme disease—relative frequency of clinical features among confirmed cases‐United States, 2008‐2019. 2021 [updated 05/03/2021]. Accessed June 24, 2021. https://www.cdc.gov/lyme/stats/graphs.html
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
