

Towards a pituitary apoplexy classification based on clinical presentation and patient journey
- PMID: 35067902
- PMCID: PMC8986731
- DOI: 10.1007/s12020-022-02983-3
Towards a pituitary apoplexy classification based on clinical presentation and patient journey
Abstract
Purpose: The condition of pituitary apoplexia contains the clinical spectre from life-threatening emergency to asymptomatic self-limiting course, which partly determines diagnostic delay and management. Outcome evaluation of course and management of pituitary apoplexia is hampered by the diverse presentation of this condition and requires appraisal. This study aimed to describe the patient journey, clinical presentation, and management of various types of pituitary apoplexy in a new classification to facilitate future outcome evaluation and identify unmet needs in the care process.
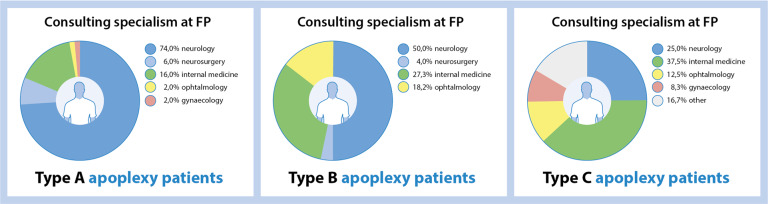
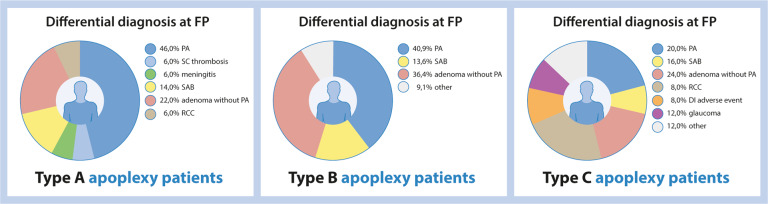
Methods: A single-center retrospective patient chart study was conducted between 2005-2021 (N = 98). Outcome measures were clinical symptoms at first presentation in hospital, being headache, consciousness, visual acuity, visual field defects (VFD), ophthalmoplegia, nausea, vomiting, fever, and hypopituitarism and care process characteristics.
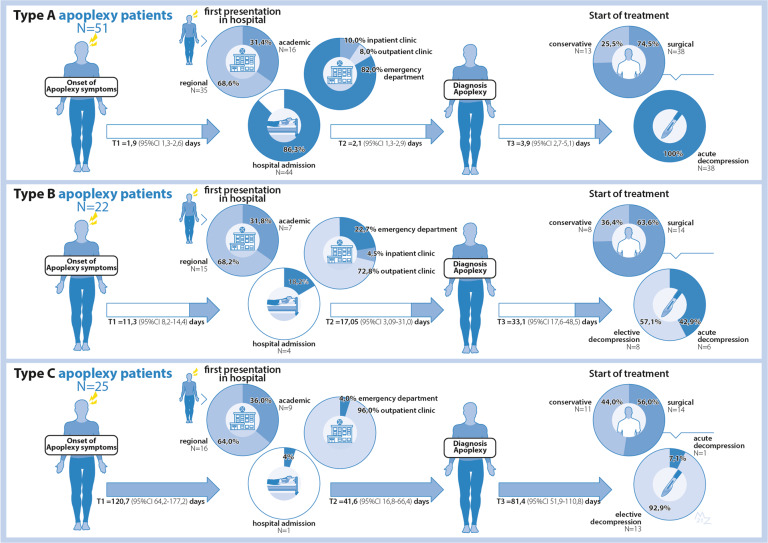
Results: Mean age was 47.6 ± 16.6 years (51.0% male). We describe their patient journey and identified three different types, differing in clinical presentation, in-hospital route, and final treatment, e.g., Acute (type A, 52%), Subacute (type B, 22.5%), and Non-acute (type C, 25.5%). Type A generally presents with acute onset headaches, VFD, or ophthalmoplegia emergency setting, with lowest mean visual acuity of both eyes and frequent hypocortisolism.
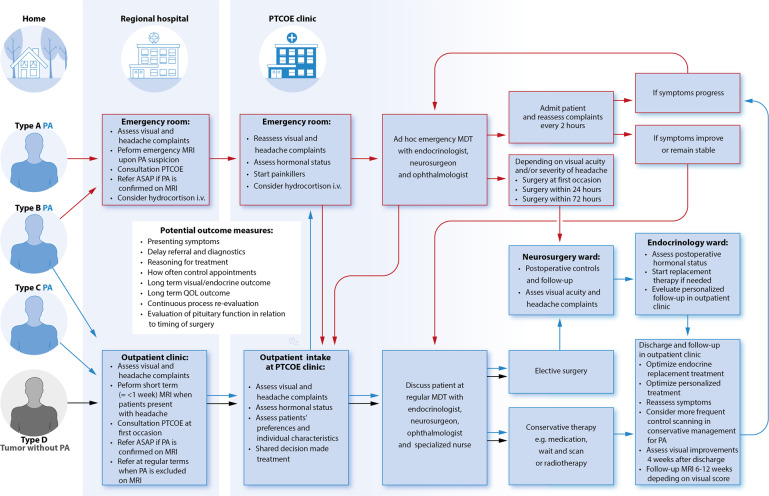
Conclusions: Pituitary apoplexy can be approached as a spectrum of disease with 3 main subtypes, with a different initial presentation, different in-hospital route resulting in different management. Acknowledging subtypes with particular needs for (emergency) referrals to Pituitary Tumors Center of Excellence (PTCOE) will serve patient care improvements, outcome evaluations and address areas for improvement.
Keywords: Acute; Classification system; Pituitary apoplexy; Spectrum of disease; Sub-acute and non-acute.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Muthukumar N. Pituitary Apoplexy: A Comprehensive Review. Neurol. India. 2020;68(Supplement):S72–s8. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
