

A Preoperative MRI-Based Radiomics-Clinicopathological Classifier to Predict the Recurrence of Pituitary Macroadenoma Within 5 Years
- PMID: 35069413
- PMCID: PMC8767054
- DOI: 10.3389/fneur.2021.780628
A Preoperative MRI-Based Radiomics-Clinicopathological Classifier to Predict the Recurrence of Pituitary Macroadenoma Within 5 Years
Abstract
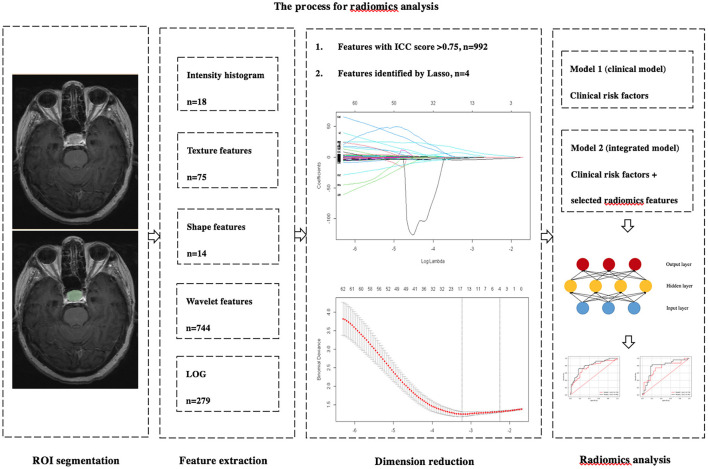
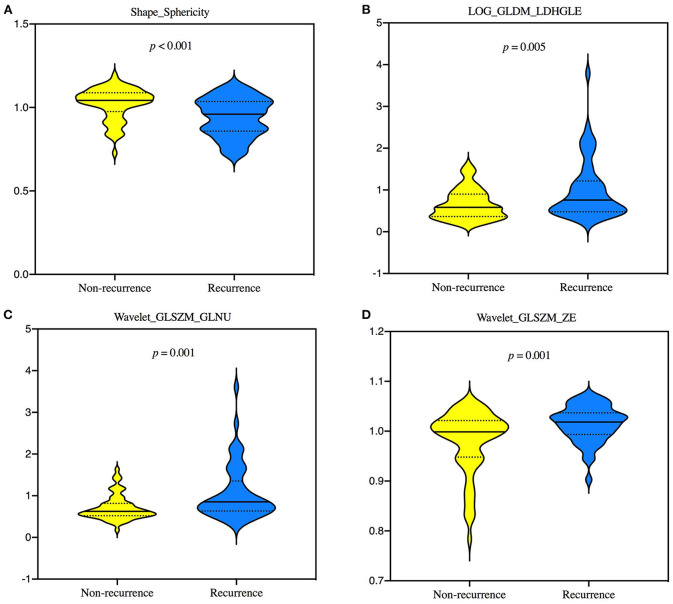
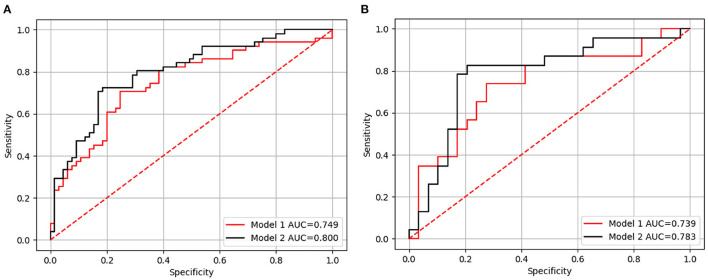
Objective: To investigate the ability of a MRI-based radiomics-clinicopathological model to predict pituitary macroadenoma (PMA) recurrence within 5 years. Materials and Methods: We recruited 74 recurrent and 94 non-recurrent subjects, following first surgery with 5-year follow-up data. Univariate and multivariate analyses were conducted to identify independent clinicopathological risk factors. Two independent and blinded neuroradiologists used 3D-Slicer software to manually delineate whole tumors using preoperative axial contrast-enhanced T1WI (CE-T1WI) images. 3D-Slicer was then used to extract radiomics features from segmented tumors. Dimensionality reduction was carried out by the least absolute shrinkage and selection operator (LASSO). Two multilayer perceptron (MLP) models were established, including independent clinicopathological risk factors (Model 1) and a combination of screened radiomics features and independent clinicopathological markers (Model 2). The predictive performance of these models was evaluated by receiver operator characteristic (ROC) curve analysis. Results: In total, 1,130 features were identified, and 4 of these were selected by LASSO. In the test set, the area under the curve (AUC) of Model 2 was superior to Model 1 {0.783, [95% confidence interval (CI): 0.718-.860] vs. 0.739, (95% CI: 0.665-0.818)}. Model 2 also yielded the higher accuracy (0.808 vs. 0.692), sensitivity (0.826 vs. 0.652), and specificity (0.793 vs. 0.724) than Model 1. Conclusions: The integrated classifier was superior to a clinical classifier and may facilitate the prediction of individualized prognosis and therapy.
Keywords: deep learning; multilayer perceptron; pituitary macroadenoma; predictive model; recurrence.
Copyright © 2022 Zhang, Luo, Kong, Wan, Long and Ma.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
[The value of conventional magnetic resonance imaging based radiomic model in predicting the texture of pituitary macroadenoma].Zhonghua Yi Xue Za Zhi. 2020 Dec 8;100(45):3626-3631. doi: 10.3760/cma.j.cn112137-20200511-01511. Zhonghua Yi Xue Za Zhi. 2020. PMID: 33333688 Chinese.
-
Preoperative classification of primary and metastatic liver cancer via machine learning-based ultrasound radiomics.Eur Radiol. 2021 Jul;31(7):4576-4586. doi: 10.1007/s00330-020-07562-6. Epub 2021 Jan 14. Eur Radiol. 2021. PMID: 33447862
-
Noncontrast Magnetic Resonance Radiomics and Multilayer Perceptron Network Classifier: An approach for Predicting Fibroblast Activation Protein Expression in Patients With Pancreatic Ductal Adenocarcinoma.J Magn Reson Imaging. 2021 Nov;54(5):1432-1443. doi: 10.1002/jmri.27648. Epub 2021 Apr 22. J Magn Reson Imaging. 2021. PMID: 33890347
-
MRI-based radiomics signature for pretreatment prediction of pathological response to neoadjuvant chemotherapy in osteosarcoma: a multicenter study.Eur Radiol. 2021 Oct;31(10):7913-7924. doi: 10.1007/s00330-021-07748-6. Epub 2021 Mar 30. Eur Radiol. 2021. PMID: 33825032
-
Pretreatment MR imaging radiomics signatures for response prediction to induction chemotherapy in patients with nasopharyngeal carcinoma.Eur J Radiol. 2018 Jan;98:100-106. doi: 10.1016/j.ejrad.2017.11.007. Epub 2017 Nov 14. Eur J Radiol. 2018. PMID: 29279146
Cited by
-
Radiomics of pituitary adenoma using computer vision: a review.Med Biol Eng Comput. 2024 Dec;62(12):3581-3597. doi: 10.1007/s11517-024-03163-3. Epub 2024 Jul 16. Med Biol Eng Comput. 2024. PMID: 39012416 Free PMC article.
-
A Novel Magnetic Resonance Imaging-Based Radiomics and Clinical Predictive Model for the Regrowth of Postoperative Residual Tumor in Non-Functioning Pituitary Neuroendocrine Tumor.Medicina (Kaunas). 2023 Aug 23;59(9):1525. doi: 10.3390/medicina59091525. Medicina (Kaunas). 2023. PMID: 37763643 Free PMC article.
-
Current status of artificial intelligence technologies in pituitary adenoma surgery: a scoping review.Pituitary. 2024 Apr;27(2):91-128. doi: 10.1007/s11102-023-01369-6. Epub 2024 Jan 6. Pituitary. 2024. PMID: 38183582
-
Machine learning method based on radiomics help differentiate posterior pituitary tumors from pituitary neuroendocrine tumors and craniopharyngioma.Sci Rep. 2025 Jun 6;15(1):19967. doi: 10.1038/s41598-025-05143-5. Sci Rep. 2025. PMID: 40481169 Free PMC article.
-
Preoperative prediction of lymphovascular invasion in patients with T1 breast invasive ductal carcinoma based on radiomics nomogram using grayscale ultrasound.Front Oncol. 2022 Dec 7;12:1071677. doi: 10.3389/fonc.2022.1071677. eCollection 2022. Front Oncol. 2022. PMID: 36568215 Free PMC article.
References
LinkOut - more resources
Full Text Sources