

Endoscopic or percutaneous biliary drainage in hilar cholangiocarcinoma: When and how?
- PMID: 35070041
- PMCID: PMC8713328
- DOI: 10.4251/wjgo.v13.i12.2050
Endoscopic or percutaneous biliary drainage in hilar cholangiocarcinoma: When and how?
Abstract
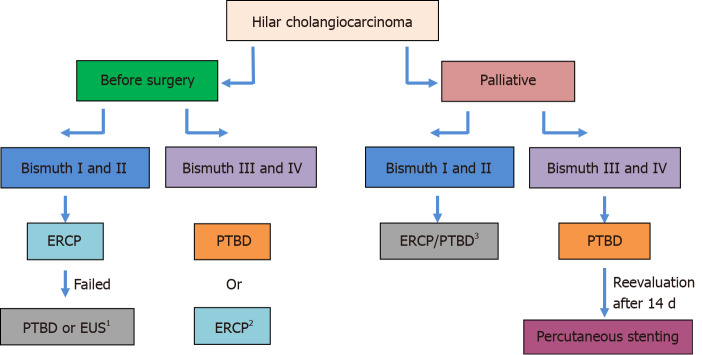
Hilar cholangiocarcinoma (hCCA) is a primary liver tumor associated with a dim prognosis. The role of preoperative and palliative biliary drainage has long been debated. The most common techniques are endoscopic retrograde cholangiopancreatography (ERCP) and percutaneous transhepatic biliary drainage (PTBD); however, recently developed endoscopic ultrasound-assisted methods are gaining more atention. Selecting the best available method in any specific scenario is crucial, yet sometimes challenging. Thus, this review aimed to discuss the available techniques, indications, perks, pitfalls, and timing-related issues in the management of hCCA. In a preoperative setting, PTBD appears to have some advantages: low risk of postprocedural complications (namely cholangitis) and better priming for surgery. For palliative purposes, we propose ERCP/PTBD depending on the experience of the operators, but also on other factors: the level of bilirubin (if very high, rather PTBD), length of the stenosis and the presence of cholangitis (PTBD), ERCP failure, or altered biliary anatomy.
Keywords: Endoscopic biliary drainage; Endoscopic ultrasound biliary drainage; Hilar cholangiocarcinoma; Percutaneous biliary drainage; Surgical oncology.
©The Author(s) 2021. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors have nothing to disclose.
Figures
References
-
- Shaib Y, El-Serag HB. The epidemiology of cholangiocarcinoma. Semin Liver Dis. 2004;24:115–125. - PubMed
-
- Chen XP, Lau WY, Huang ZY, Zhang ZW, Chen YF, Zhang WG, Qiu FZ. Extent of liver resection for hilar cholangiocarcinoma. Br J Surg. 2009;96:1167–1175. - PubMed
-
- Jonas S, Thelen A, Benckert C, Biskup W, Neumann U, Rudolph B, Lopez-Häänninen E, Neuhaus P. Extended liver resection for intrahepatic cholangiocarcinoma: A comparison of the prognostic accuracy of the fifth and sixth editions of the TNM classification. Ann Surg. 2009;249:303–309. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
