

Comparison of National Comprehensive Cancer Network and European Position Statement protocols for nodule management in low-dose computed tomography lung cancer screening in a general Chinese population
- PMID: 35070370
- PMCID: PMC8743405
- DOI: 10.21037/jtd-21-1312
Comparison of National Comprehensive Cancer Network and European Position Statement protocols for nodule management in low-dose computed tomography lung cancer screening in a general Chinese population
Abstract
Background: Low-dose computed tomography (LDCT) lung cancer screening often refers individuals to unnecessary examinations. This study aims to compare the European Position Statement (EUPS) and National Comprehensive Cancer Network (NCCN) protocols in management of participants at baseline screening round.
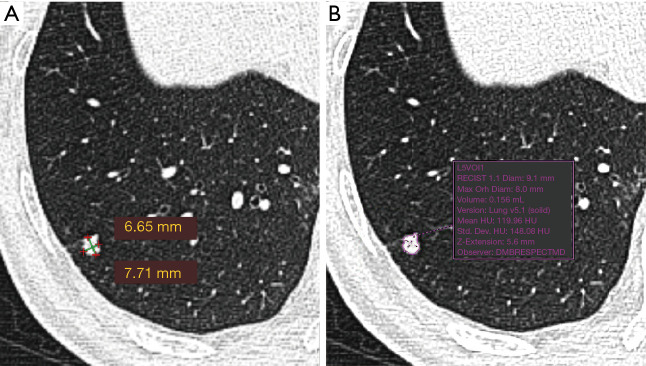
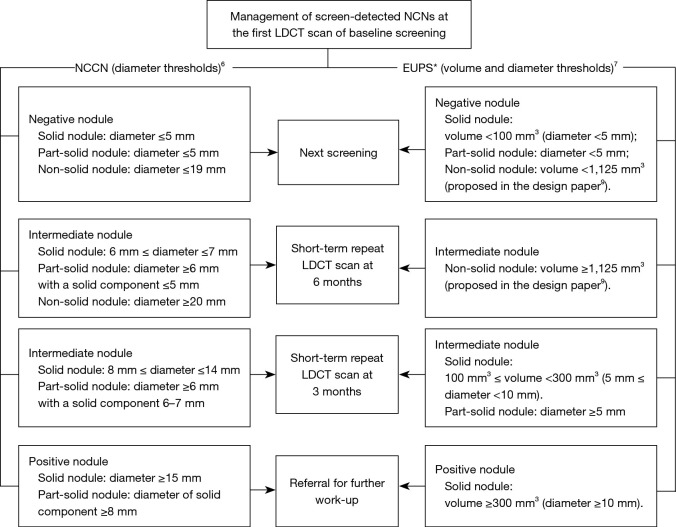
Methods: LDCT lung cancer screening was prospectively performed in a Chinese asymptomatic population aged 40-74 years. A total of 1,000 consecutive baseline LDCT scans were read twice independently. All screen-detected lung nodules by the first reader were included. The first reader manually measured the diameter of lung nodules (NCCN protocol), and the second reader semi-automatically measured the volume and diameter (EUPS volume and diameter protocols). The protocols were used to classify the participants into three management groups: next screening round, short-term repeat LDCT scan and referral to a pulmonologist. Groups were compared using Wilcoxon test for paired samples. Number of lung cancers by protocols was provided.
Results: Of the 1,000 participants (61.4±6.7 years old), 168 lung nodules in 124 participants were visually detected and manually measured in the first reading, and re-measured semi-automatically. Applying the NCCN protocol, EUPS volume and diameter protocol, the proportion of referrals among all participants was 0.6%, 1.9%, and 1.4%, respectively. The proportion of short-term repeat scans was 4.5%, 9.7% and 4.5%, respectively. Among the 10 lung cancer patients, one would have been diagnosed earlier if the EUPS volume protocol would have been followed.
Conclusions: In a first round screening in a Chinese general population, the lower threshold for referral in the EUPS protocol as compared to the NCCN protocol, leads to more referrals to a pulmonologist, with the potential of earlier cancer diagnosis. The EUPS volume protocol recommends fewer participants to short-term repeat LDCT scan than the EUPS diameter protocol. Follow-up studies should show the impact of both protocols on (interval) cancer diagnosis.
Keywords: Lung nodule; diameter; low-dose computed tomography (LDCT); mass screening; volume.
2021 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://dx.doi.org/10.21037/jtd-21-1312). The authors have no conflicts of interest to declare.
Figures

References
-
- American College of Radiology. Lung Rads. Available online: https://www.acr.org/Clinical-Resources/Reporting-and-Data-Systems/Lung-Rads
LinkOut - more resources
Full Text Sources