

Prediction of late recurrence after radiofrequency ablation of HBV-related hepatocellular carcinoma with the age-male-albumin-bilirubin-platelets (aMAP) risk score: a multicenter study
- PMID: 35070419
- PMCID: PMC8748026
- DOI: 10.21037/jgo-21-506
Prediction of late recurrence after radiofrequency ablation of HBV-related hepatocellular carcinoma with the age-male-albumin-bilirubin-platelets (aMAP) risk score: a multicenter study
Abstract
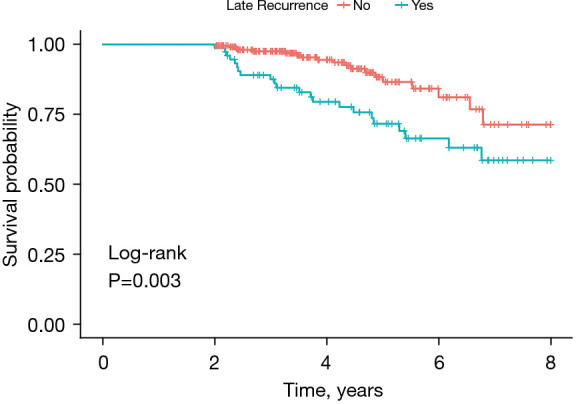
Background: Long-term survivals of patients with HBV-related hepatocellular carcinoma are limited by the high incidence of tumor recurrence after radiofrequency ablation (RFA), identification of the risk factors and understanding the patterns of recurrence can help to improve the comprehensive management of patients after RFA. Therefore, the purpose of the study is to explore the prognostic value of the age-male-albumin-bilirubin-platelets (aMAP) score in patients with early-stage HBV-related hepatocellular carcinoma (HCC) receiving RFA; investigate the risk factors and patterns of late recurrence (LR); and develop a nomogram to predict recurrence-free survival (RFS).
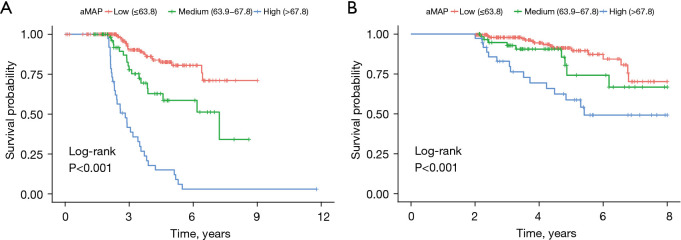
Methods: A retrospective review of HBV-related HCC patients who underwent primary RFA from March 2012 to December 2020 was conducted. The prognostic value of the aMAP score was evaluated in a primary cohort (n=302) and then further validated in an independent validation cohort (n=143). The optimal threshold of aMAP scores was calculated by X-tile 3.6.1 software. A prognostic nomogram was constructed from multivariate analysis and validated in an external validation cohort.
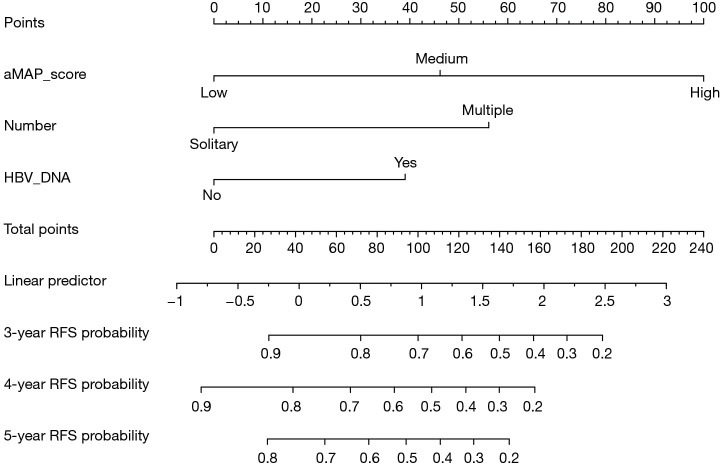
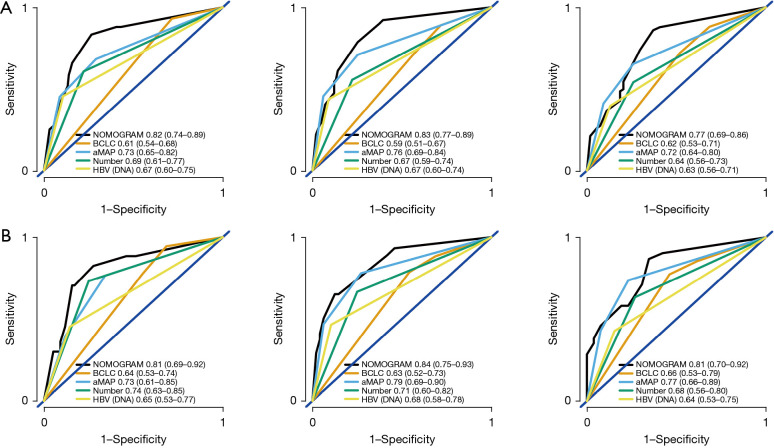
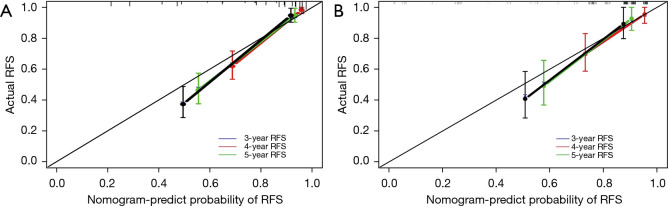
Results: Patients with aMAP scores ≤63.8, 63.8-67.8, and >67.8 were classified into low-, medium-, and high-recurrence risk groups, respectively. The C-index to predict LR was 0.76 (95% CI: 0.700-0.810). The high-risk group was associated with the worst RFS (HR: 5.298; 95% CI, 2.697-10.408; P<0.001) and overall survival (OS) (HR: 2.639; 95% CI, 1.097-6.344; P=0.03) compared with medium- and low-risk groups. The aMAP score, multiple tumors and preoperative HBV DNA level were independent risk factors for LR. The proposed nomogram had excellent performance in predicting LR of HBV-related HCC [C-index: 0.82 (95% CI: 0.772-0.870)].
Conclusions: This study demonstrated that the aMAP score can serve as an objective predictor of LR for HBV-related HCC patients after RFA. The nomogram based on preoperative HBV DNA level, aMAP score, and number of tumors can reliably help clinicians to stratify the recurrence risk of HCC patients after RFA.
Keywords: HBV-related hepatocellular carcinoma; aMAP score; radiofrequency ablation; recurrence.
2021 Journal of Gastrointestinal Oncology. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://dx.doi.org/10.21037/jgo-21-506). The authors have no conflicts of interest to declare.
Figures
References
-
- European Association for the Study of the Liver . Electronic address: easloffice@easloffice.eu; European Association for the Study of the Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J Hepatol 2017;67:370-98. 10.1016/j.jhep.2017.03.021 - DOI - PubMed
LinkOut - more resources
Full Text Sources